What Is the Difference Between Hyperpigmentation and Hypopigmentation?
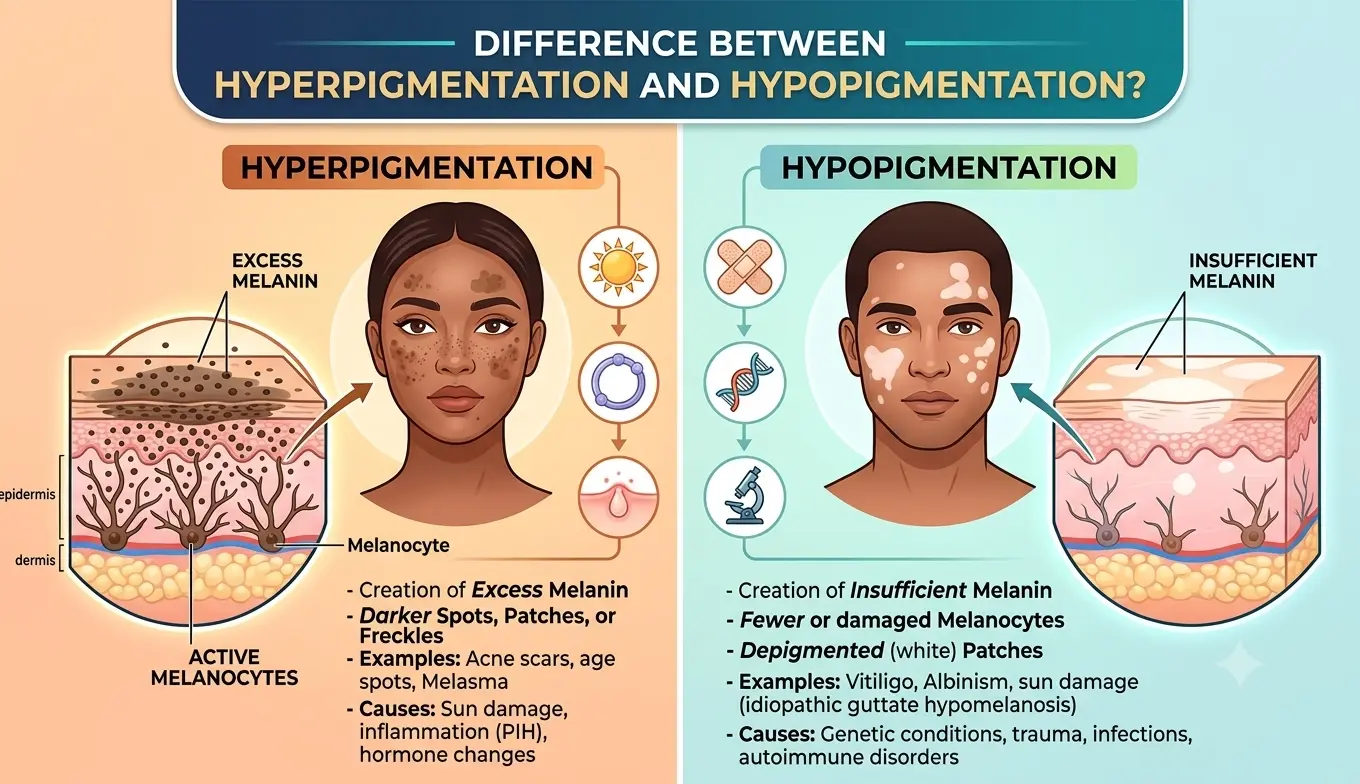
Hyperpigmentation and hypopigmentation are opposite ends of the same spectrum: both involve an abnormality in the skin’s melanin production, but they produce entirely different visual outcomes and require different clinical approaches. Hyperpigmentation refers to areas where too much melanin has been produced, resulting in skin that appears darker than the surrounding tissue. Hypopigmentation refers to areas where too little melanin has been produced, resulting in skin that appears lighter or paler than the surrounding tissue. Most of the pigmentation concerns treated in aesthetic practice involve hyperpigmentation, including age spots, post-inflammatory hyperpigmentation, and melasma, and these are the presentations that professional resurfacing with a treatment such as the Trexyne Peel can support. Hypopigmentation is a separate category of concern with different causes and different management considerations, and distinguishing between the two clearly is the starting point for any appropriate clinical conversation about skin tone.
Understanding Hyperpigmentation
Hyperpigmentation develops when melanocytes, the cells responsible for producing the pigment melanin, produce more melanin than the skin requires in a given area. This excess melanin deposits within the epidermis, and in some cases the dermis, producing darker patches or spots that contrast with the surrounding skin.
The triggers for hyperpigmentation vary considerably and determine both the type of hyperpigmentation present and how it should be treated. UV radiation is the most common trigger, producing the solar lentigines commonly known as age spots in areas with high lifetime sun exposure. Hormonal changes, particularly elevated oestrogen and progesterone, produce melasma through a mechanism that sensitises melanocytes to UV stimulus. Inflammation triggers post-inflammatory hyperpigmentation by stimulating melanocyte overproduction during the skin’s repair response to acne, trauma, or treatment reactions.
What these different forms of hyperpigmentation share is that they all involve an overactive melanin response. The treatment approach for each type is shaped by the underlying trigger, but the general principle, supporting the progressive displacement of excess melanin through accelerated cell turnover, applies across the hyperpigmentation category. This is why professional resurfacing is a central tool in hyperpigmentation management.
Understanding Hypopigmentation
Hypopigmentation is the opposite condition. Instead of excess melanin, the affected area has reduced or absent melanin, producing skin that appears lighter or paler than the surrounding tissue. The skin in hypopigmented areas may range from slightly lighter than baseline to completely without colour, depending on the cause and severity.
Hypopigmentation can be caused by a range of factors. Some are congenital, meaning they are present from birth, such as albinism, which involves a genetic absence of melanin production across the entire body, or piebaldism, which affects specific areas. Some are acquired during a person’s lifetime through trauma, inflammation, or disease processes.
Post-inflammatory hypopigmentation can develop following significant skin trauma, burns, certain infections, or aggressive treatments that have damaged the melanocytes in the affected area. Unlike post-inflammatory hyperpigmentation, where excess melanin is produced as a response to inflammation, post-inflammatory hypopigmentation occurs when the melanocytes themselves have been damaged or destroyed by the inflammatory process, leaving them unable to produce adequate melanin during the healing phase.
Vitiligo is the most widely recognised cause of acquired hypopigmentation. It is an autoimmune condition in which the immune system attacks and destroys melanocytes in specific areas of the skin, producing well-defined patches of depigmented skin that have lost colour entirely rather than just becoming lighter.
Why They Require Different Clinical Approaches
The fundamental difference between hyperpigmentation and hypopigmentation in clinical terms is the state of the melanocytes responsible for the affected area. In hyperpigmentation, the melanocytes are overactive and producing too much melanin. In hypopigmentation, the melanocytes are underactive, damaged, or absent, and producing too little.
This difference shapes every clinical decision that follows. Resurfacing treatments, including the Trexyne Peel, work by stimulating cell turnover and supporting the gradual displacement of excess melanin from the epidermis. This approach is directly relevant to hyperpigmentation, where there is excess melanin to displace. It is not appropriate as a primary treatment for hypopigmentation, where the concern is the absence or insufficiency of melanin rather than its excess. Resurfacing skin that lacks melanin does not restore melanin production, and applying aggressive treatments to hypopigmented areas can risk further damage to any remaining melanocyte function.
The clinical pathway for hypopigmentation is therefore fundamentally different from the pathway for hyperpigmentation, and accurate identification of which condition is present is the essential first step in any consultation about skin tone concerns.
How to Distinguish Them Clinically
In most cases, the clinical distinction between hyperpigmentation and hypopigmentation is straightforward based on visual assessment: hyperpigmented areas are darker than the surrounding skin, while hypopigmented areas are lighter.
However, context and careful observation are important. In very fair skin, mild hypopigmentation may be less obvious than in medium or darker skin, where the contrast between pigmented and depigmented skin is much more visible. In skin recovering from a recent inflammatory event, distinguishing between a reddish PIH mark and a hypopigmented patch that appears pale against inflamed surrounding skin can require careful assessment.
Asking about the client’s history is the most reliable way to contextualise what is being observed. Has the area been darker than baseline, suggesting hyperpigmentation, or lighter? Was there a specific event, such as a burn, a severe inflammatory reaction, or a significant skin infection, that might have damaged melanocytes and produced hypopigmentation? Is the pattern bilateral and symmetrical, suggesting a systemic hormonal influence, or localised to a specific area consistent with a local injury or inflammation?
For presentations that could represent vitiligo or another systemic autoimmune condition, or where the clinical picture is unclear, referral to a dermatologist for assessment is appropriate before any aesthetic intervention is considered.
The Most Common Hyperpigmentation Types in Aesthetic Practice
The vast majority of pigmentation concerns encountered in aesthetic skincare practice fall within the hyperpigmentation category. Understanding the most common types helps practitioners provide accurate information to clients and design appropriate treatment protocols.
Solar lentigines, commonly called age spots or liver spots, are flat, defined darker patches produced by cumulative UV exposure over years. They are most common on the face, hands, and décolleté and tend to deepen and multiply with age and continued UV exposure without photoprotection.
Post-inflammatory hyperpigmentation leaves flat, dark marks at the site of previous inflammation. Acne is the most common cause in aesthetic practice, but PIH can follow any inflammatory event including insect bites, eczema flares, contact reactions, and treatments that generated an excessive inflammatory response in susceptible skin.
Melasma is a hormonally influenced pattern of hyperpigmentation characterised by bilateral, diffuse patches across the central face. It is driven by a combination of hormonal sensitivity and UV exposure and is particularly associated with pregnancy, hormonal contraception, and perimenopause.
Freckles, or ephelides, are small, flat, concentrated melanin deposits determined largely by genetics and activated by UV exposure. They are most common in lighter skin types and fair-haired individuals and tend to fade during winter and deepen in summer.
Where the Trexyne Peel Fits in Hyperpigmentation Management
The Trexyne Peel is a professional resurfacing treatment relevant to hyperpigmentation management across multiple presentation types. Its mechanical resurfacing mechanism using marine-algae spicules stimulates cell turnover without chemical exfoliants, supporting the progressive displacement of excess epidermal melanin over a course of professional sessions.
For post-inflammatory hyperpigmentation in particular, the mechanical mechanism is clinically relevant because it avoids the chemical inflammatory trigger that can provoke further PIH in susceptible skin. Clients whose hyperpigmentation was itself caused by inflammation are at risk of having that pigmentation worsened by resurfacing treatments that generate a significant chemical inflammatory response. The Trexyne Peel’s approach reduces this risk by removing the chemical trigger from the resurfacing mechanism.
For solar lentigines and photodamage-related hyperpigmentation, a sustained mechanical resurfacing course supports the gradual renewal of the epidermal layers where the accumulated melanin deposits sit. The tiered protocol allows intensity to be matched to the depth and extent of the pigmentation and progressively advanced as the skin demonstrates its tolerance.
Stabilised Vitamin E in the formulation supports recovery throughout the treatment course, helping the skin manage the inter-session period efficiently and reducing the residual inflammatory load that could otherwise trigger further melanocyte activity in susceptible skin.
Hypopigmentation and the Importance of Accurate Assessment
Hypopigmentation presentations require careful clinical assessment before any treatment is recommended, and aesthetic resurfacing is generally not a primary intervention for hypopigmented conditions. The most important clinical priority for hypopigmentation is accurate diagnosis of the underlying cause, since different causes have very different implications for management.
Vitiligo requires a different management approach from post-inflammatory hypopigmentation. Congenital hypopigmentation involving absent melanocytes requires different considerations from acquired hypopigmentation where some melanocyte function may remain. Certain topical and light-based treatments have been explored in the management of vitiligo and other hypopigmentation conditions, but these are specialist dermatological territory rather than standard aesthetic practice.
Practitioners who encounter hypopigmented areas in clients presenting for aesthetic treatment should assess whether the hypopigmentation is a separate, pre-existing condition or whether it is related to the concern the client is seeking treatment for. Any doubt about the nature, cause, or extent of hypopigmentation warrants dermatological referral before aesthetic treatment proceeds in the affected area.
Practitioners interested in exploring the Trexyne Peel for their hyperpigmentation protocols can find full product information and supply options through the Trexyne shop, or contact the team directly via the Trexyne contact page.
More information on the Trexyne approach to professional botanical resurfacing is available on the Trexyne website.
Conclusion
Hyperpigmentation and hypopigmentation are opposite melanin abnormalities that produce darker and lighter areas respectively. Hyperpigmentation, which includes age spots, post-inflammatory hyperpigmentation, melasma, and related conditions, is the category most commonly addressed in aesthetic practice and the one that professional resurfacing directly supports. Hypopigmentation, which includes vitiligo and post-inflammatory depigmentation, involves reduced or absent melanin production and requires a fundamentally different clinical approach. Distinguishing between the two accurately at consultation is essential before any treatment plan is designed. For hyperpigmentation, the Trexyne Peel offers a mechanical resurfacing mechanism that supports progressive displacement of excess epidermal melanin without chemical inflammatory triggers, with stabilised Vitamin E for recovery and a tiered protocol that adapts to the individual’s skin and concern. For clients managing hyperpigmentation concerns, this approach may support a brighter, more even-looking complexion over the course of a well-managed professional treatment programme.
FAQs
Q: What is the difference between hyperpigmentation and hypopigmentation?
Hyperpigmentation involves areas where too much melanin has been produced, making the skin appear darker than surrounding tissue. Hypopigmentation involves areas where too little melanin has been produced, making the skin appear lighter or paler. They are opposite conditions caused by different mechanisms and requiring different clinical approaches.
Q: Can the Trexyne Peel help with hyperpigmentation?
Yes. The Trexyne Peel supports hyperpigmentation management by stimulating cell turnover through a mechanical resurfacing mechanism that encourages the progressive displacement of excess epidermal melanin. It is relevant for post-inflammatory hyperpigmentation, solar lentigines, and photodamage-related pigmentation, and its non-chemical mechanism reduces the risk of provoking further pigmentation in susceptible skin types.
Q: Can the Trexyne Peel treat hypopigmentation?
No. The Trexyne Peel is designed for professional resurfacing to support cell turnover and address excess epidermal pigmentation. It is not a treatment for hypopigmentation, which involves reduced or absent melanin production rather than excess. Hypopigmentation conditions including vitiligo require specialist assessment and different management approaches.
Q: What causes hypopigmentation?
Hypopigmentation can be caused by genetic conditions affecting melanin production, post-inflammatory depigmentation where melanocytes have been damaged or destroyed by a severe inflammatory event, or autoimmune conditions such as vitiligo where the immune system attacks melanocytes. Each cause has different implications for management and prognosis.
Q: Is post-inflammatory hyperpigmentation the same as post-inflammatory hypopigmentation?
No. Post-inflammatory hyperpigmentation occurs when inflammation stimulates excess melanin production, leaving darker marks. Post-inflammatory hypopigmentation occurs when inflammation damages the melanocytes, leaving lighter patches. Both can follow significant inflammatory skin events, but they represent opposite outcomes of the melanocyte’s response to inflammation.
Q: Why is accurate diagnosis of the pigmentation type so important before treatment?
Hyperpigmentation and hypopigmentation require fundamentally different treatment approaches. Applying a resurfacing treatment designed to address excess melanin to a hypopigmented area is not appropriate and could risk further damage to any remaining melanocyte function. Accurate clinical assessment, including understanding the cause and direction of the pigmentation change, is the essential first step before any treatment is recommended.
Q: When should a client with pigmentation concerns be referred to a dermatologist?
Any client with hypopigmented areas, particularly if the pattern could suggest vitiligo or another systemic autoimmune condition, should be referred for dermatological assessment before aesthetic treatment. Clients with pigmentation that does not fit the expected appearance of common hyperpigmentation types, or that is changing in character or distribution, should also be referred rather than treated empirically without a confirmed diagnosis.