What Is Post-Inflammatory Hyperpigmentation?
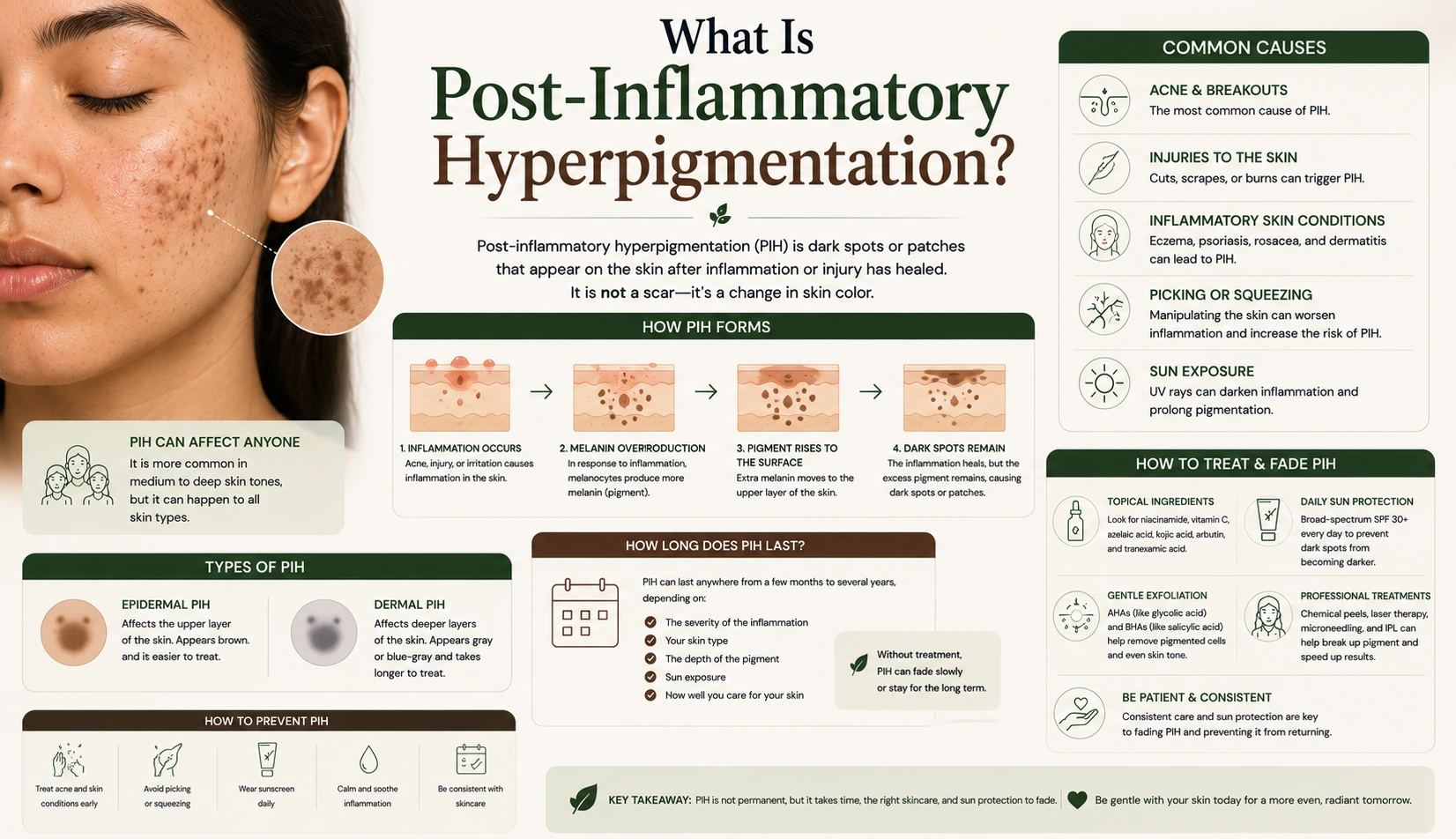
Post-inflammatory hyperpigmentation, most commonly referred to as PIH, is the flat, discoloured mark that remains on the skin after an inflammatory event has resolved. It is one of the most common pigmentation concerns seen in aesthetic practice and one of the most frequently misunderstood, both by clients and sometimes by the practitioners treating them. PIH is not a scar. It involves no structural damage to the dermis and no permanent alteration to the skin’s architecture. It is a pigmentation change that sits within the epidermis and, with the right approach, can respond meaningfully to professional resurfacing over a course of sessions. The Trexyne Peel is a relevant professional option for PIH management, offering a mechanical resurfacing mechanism that avoids the inflammatory trigger most likely to produce new PIH in susceptible skin while treating the existing marks. Understanding PIH clearly is the starting point for treating it effectively.
How Post-Inflammatory Hyperpigmentation Forms
PIH forms through a specific biological sequence that begins with inflammation rather than with UV exposure. When the skin experiences an inflammatory event, whether from an acne lesion, a skin injury, an allergic reaction, an insect bite, or a treatment that provoked more inflammatory response than the skin could manage, the inflammatory mediators released in the affected area can stimulate the melanocytes to produce excess melanin.
Melanocytes are the cells responsible for producing melanin, the pigment that gives skin its colour. Under normal circumstances, they produce melanin at a rate appropriate to the skin’s needs. When inflammation activates the local melanocyte population, this regulation is disrupted. The melanocytes produce more melanin than the area requires, and this excess pigment is deposited unevenly in the epidermal layers as the inflammation resolves and the lesion heals.
The result is a patch of darker skin at the site of the original inflammation. The colour of the mark depends on the depth of melanin deposition and the individual’s skin tone. In lighter skin types, PIH often presents as pink or reddish marks in the initial weeks, transitioning to a light brown tone as the inflammatory component fully resolves. In medium to darker skin tones, PIH tends to present as mid-brown, deep brown, or near-black patches and is typically more pronounced and longer-lasting.
Why PIH Is More Common and More Visible in Darker Skin Tones
The relationship between skin tone and PIH severity is one of the most clinically important aspects of this condition. Melanocytes in skin with higher melanin content, which corresponds broadly to Fitzpatrick types III to VI, have higher baseline activity and a stronger response to inflammatory signals. When inflammation triggers melanocyte overproduction in these skin types, the resulting pigment response is often more pronounced and more durable than the same inflammatory event would produce in lighter skin.
This does not mean PIH cannot occur in lighter skin. It can, and it does. But in lighter skin types it often appears as pinkish-red marks that reflect the vascular component of the post-inflammatory response and fade relatively quickly as the inflammation fully resolves. In medium to darker skin, the hyperpigmentation is a true melanin deposit that persists significantly longer and requires more sustained treatment to address.
This biological difference is one of the reasons treatment mechanism matters so much for clients with PIH in darker skin tones. Any treatment that generates additional inflammation in already-susceptible melanocytes risks producing new PIH even as it addresses existing marks. Selecting a resurfacing approach that minimises this inflammatory trigger is a foundational clinical decision for practitioners working with this client group.
Common Causes of Post-Inflammatory Hyperpigmentation
PIH can follow any inflammatory event in the skin, and the range of triggers is broad. Understanding the most common causes helps practitioners identify PIH accurately at consultation and distinguish it from other pigmentation types.
Acne is the most common cause of PIH seen in aesthetic practice. Each inflamed acne lesion has the potential to produce a PIH mark as it resolves, and clients who experience frequent or severe breakouts can accumulate significant pigmentation over time. The marks often follow the exact shape and location of the original lesion, which is a reliable diagnostic indicator.
Trauma to the skin, including cuts, burns, insect bites, and contact reactions, can all produce PIH at the site of the injury as the skin heals. Friction dermatitis and chronic rubbing of a specific area, such as the inner thighs or underarms, can also produce PIH through repeated low-level inflammatory trauma.
Treatments that generate an inflammatory response in the skin are a clinically significant cause of PIH, particularly in susceptible skin types. Chemical resurfacing treatments, laser procedures, waxing, and threading can all produce PIH in Fitzpatrick types III to VI if the inflammatory response generated exceeds what those melanocytes can manage without overproducing pigment. This is why treatment mechanism selection and careful assessment of a client’s PIH risk before any in-clinic procedure is part of responsible aesthetic practice.
Skin conditions including eczema, psoriasis, and contact dermatitis can also leave PIH marks in areas where they have been active, particularly after flare-ups. Managing these underlying conditions appropriately before considering resurfacing is important, as ongoing inflammatory activity from an uncontrolled skin condition will continue to produce new PIH during any treatment course.
How to Identify PIH in a Clinical Assessment
Accurate identification of PIH at consultation is the foundation of an appropriate treatment plan. Several features help confirm PIH as the diagnosis rather than other forms of pigmentation.
The mark is flat. This is the most reliable and consistently useful distinguishing feature. PIH involves no structural change to the skin. Running a clean finger lightly over the surface of a PIH mark reveals no textural difference from the surrounding skin. This distinguishes it from atrophic acne scars, which are palpable as depressions, and from raised hypertrophic scars or keratosis pilaris, which are elevated.
The mark’s location corresponds to a previous or current inflammatory event. A client who reports a recent breakout in a specific area and now has a dark mark in the same location has almost certainly produced PIH from that breakout. A client with eczema who has a dark patch on their arm in the same location as a recent flare has the same presentation.
The colour is generally even within the mark, ranging from pink to brown or near-black depending on skin tone and the depth of melanin deposition. Marks with very uneven colour, irregular borders, or patterns inconsistent with the reported history should be assessed more carefully before assuming PIH.
The mark is relatively recent in relation to the reported inflammatory event. PIH marks typically become visible within days to weeks of the inflammation that caused them, not months or years later without any interim trigger.
How PIH Differs From Other Pigmentation Types
PIH is one of several distinct pigmentation presentations that practitioners encounter, and distinguishing it from others shapes the treatment approach.
Unlike solar lentigines, or age spots, PIH does not require UV exposure as its primary trigger. It can develop on any area of the body that has experienced inflammation, including areas that rarely see sun, such as the torso or legs.
Unlike melasma, PIH does not have a hormonal driver. It is a response to a specific local inflammatory event rather than a systemic hormonal change that sensitises melanocytes across a broader area of the face. Melasma tends to present with bilateral symmetry across the central face and fluctuates with UV exposure and hormonal cycles. PIH follows the location of the original inflammation and does not typically fluctuate seasonally.
Unlike structural acne scarring, PIH involves no dermal damage. It is entirely an epidermal change and as such responds to resurfacing treatments in a way that structural scars do not.
How Professional Resurfacing Addresses PIH
PIH responds to professional resurfacing because the pigment sits within the epidermis, where accelerated cell turnover can progressively displace pigmented cells with fresh, unpigmented ones over a course of sessions. Each resurfacing session stimulates this renewal, and the cumulative effect across a sustained course produces a gradual, visible fading of the marks.
The Trexyne Peel is particularly well suited to PIH management because its mechanical resurfacing mechanism does not generate a chemical inflammatory response. For PIH-prone skin, this means the resurfacing stimulus supports renewal without activating the same inflammatory pathway that produced the original pigmentation. The risk of producing new PIH during treatment, which is a genuine concern with chemical resurfacing in susceptible skin types, is significantly reduced by removing the chemical inflammatory trigger from the mechanism entirely.
Stabilised Vitamin E in the formulation supports recovery, reducing the post-treatment window during which recovering skin is most vulnerable to inflammatory triggers that could provoke further melanocyte activity. The tiered protocol allows conservative progression suited to skin that has already demonstrated a tendency towards PIH.
Practitioners looking to incorporate a professional resurfacing option for PIH management into their treatment offering can explore the full range via the Trexyne shop, or contact the team directly through the Trexyne contact page.
The Essential Role of Daily SPF in PIH Management
Daily broad-spectrum sun protection is not supplementary advice for clients managing PIH. It is a clinical requirement. UV exposure amplifies melanocyte activity in the affected areas and can deepen existing PIH marks, produce new ones, and counteract the progressive improvement being achieved through professional resurfacing.
Without consistent daily SPF use throughout a treatment course, every session of resurfacing is working against ongoing UV-driven melanocyte stimulation. The net effect is slower progress, less visible improvement, and a higher likelihood that results plateau before the client has achieved the degree of improvement they came in for.
Broad-spectrum protection covering both UVA and UVB should be applied every morning without exception. UVA is present year-round at relatively consistent levels regardless of cloud cover and penetrates glass, meaning incidental exposure through car journeys and indoor proximity to windows contributes to the UV load the skin is managing even on apparently cloudy days.
What Realistic Improvement in PIH Looks Like
PIH responds well to professional resurfacing when the treatment mechanism, the session spacing, and the client’s aftercare all align correctly. Visible improvement in the depth and intensity of the marks tends to build progressively across the course, with the most noticeable changes often becoming apparent in the middle sessions rather than immediately after the first.
The timeline varies by the age and depth of the pigmentation, the individual’s cell turnover rate, and how consistently sun protection is maintained between sessions. Recent, superficial PIH may show meaningful fading within a few sessions. Older, more established marks that have been present for months or years without treatment take longer to address, as the melanin is distributed more densely and the renewal cycle needs to work through more layers of accumulated pigmented cells.
More information on the Trexyne approach to professional botanical resurfacing is available on the Trexyne website.
Conclusion
Post-inflammatory hyperpigmentation is a flat, epidermal pigmentation change produced when the skin’s melanocytes overproduce melanin in response to an inflammatory event. It is more common and more pronounced in medium to darker skin tones, where melanocyte activity and inflammatory melanin responses are stronger. PIH can follow acne, trauma, skin conditions, and treatments that generate inflammatory responses in susceptible skin. It differs from structural scarring, melasma, and solar lentigines in its cause, its appearance, and its clinical behaviour. Professional resurfacing supports PIH improvement by accelerating cell turnover and progressively displacing pigmented cells. The Trexyne Peel addresses PIH through a mechanical mechanism that avoids the chemical inflammatory trigger most likely to worsen the condition in susceptible skin, supported by stabilised Vitamin E for recovery and a tiered protocol suited to gradual, well-managed progression. With consistent daily SPF and appropriate treatment spacing, it may support meaningful, visible improvement in PIH and contribute to a brighter, more even-looking complexion over the course of a sustained professional treatment plan.
FAQs
Q: What is post-inflammatory hyperpigmentation?
Post-inflammatory hyperpigmentation is the flat, discoloured mark left on the skin after an inflammatory event such as an acne lesion, skin injury, or a treatment that provoked an inflammatory response. It forms when inflammation stimulates melanocytes to produce excess melanin in the affected area. It is entirely within the epidermis and involves no structural damage to the skin.
Q: Is post-inflammatory hyperpigmentation the same as a scar?
No. PIH is a pigmentation change with no structural component. The skin surface is completely flat over a PIH mark, with no depression or elevation. Acne scars involve structural damage to the dermis where collagen has been disrupted. Both can appear after acne, but they require different treatment approaches.
Q: Why is PIH worse in darker skin tones?
Darker skin tones have higher baseline melanocyte activity and a stronger melanin response to inflammatory signals. When inflammation triggers melanocyte overproduction in these skin types, the resulting pigmentation is typically more pronounced, darker, and longer-lasting than the same inflammatory event would produce in lighter skin. This makes treatment mechanism selection particularly important for these clients.
Q: Can professional resurfacing help with post-inflammatory hyperpigmentation?
Yes. PIH sits within the epidermis, where accelerated cell turnover progressively displaces pigmented cells with fresh, unpigmented ones. A course of professional resurfacing can produce meaningful visible fading over time. For PIH-prone skin, a mechanical resurfacing approach that avoids chemical inflammatory triggers reduces the risk of producing new pigmentation during treatment.
Q: How long does post-inflammatory hyperpigmentation last?
The timeline depends on the depth and age of the pigmentation, the individual’s skin tone, and how consistently daily SPF is used. Recent, superficial PIH may begin to fade within weeks with appropriate management. Older or more established marks, particularly in medium to darker skin tones, can persist for months to years without professional intervention.
Q: Does the Trexyne Peel help with PIH?
The Trexyne Peel supports PIH improvement through a mechanical resurfacing mechanism that stimulates cell turnover without generating the chemical inflammatory response most likely to worsen PIH in susceptible skin. Stabilised Vitamin E supports recovery, and the tiered protocol allows conservative, gradual progression suited to skin that has demonstrated a tendency towards post-inflammatory pigmentation.
Q: Why is daily SPF so important for treating PIH?
UV exposure amplifies melanocyte activity in areas affected by PIH, deepening existing marks and producing new ones. Without consistent daily broad-spectrum SPF use, professional resurfacing works against ongoing UV-driven pigmentation. SPF is a clinical requirement for PIH treatment to produce and sustain visible results, not simply general skincare advice.