What Is the Difference Between Acne Scarring and Acne Dark Marks?
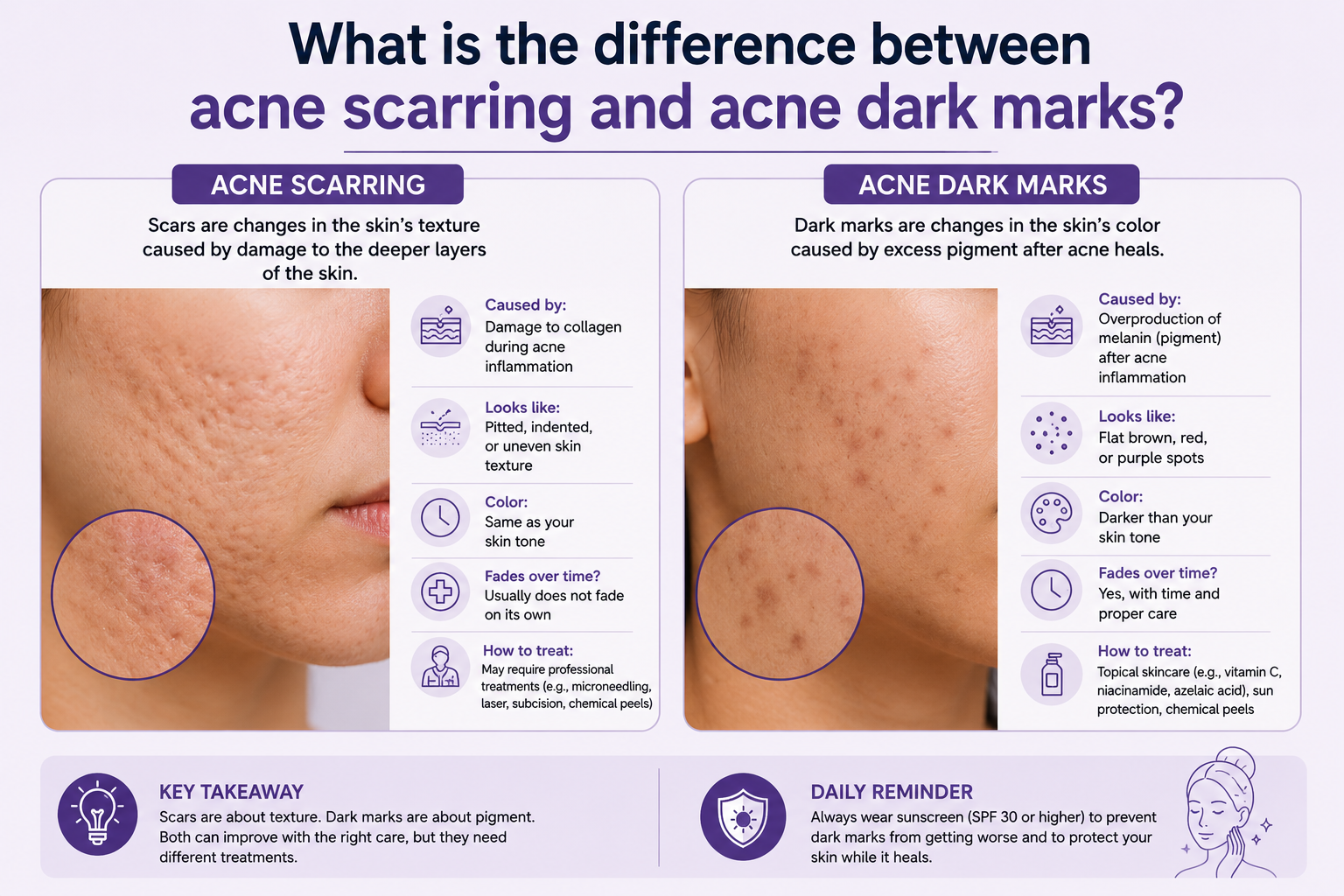
Acne scarring and acne dark marks are two distinct conditions, and the difference between them matters enormously when it comes to treatment. Dark marks, clinically known as post-inflammatory hyperpigmentation, are a pigmentation change caused by inflammation. They sit within the skin’s surface layers and, with the right approach, can respond well to professional resurfacing. Acne scars, by contrast, involve structural changes to the dermis, the deeper layer of the skin, where collagen has been permanently disrupted. These require different treatment strategies entirely. The confusion between the two is understandable because both follow acne, both leave visible marks, and both take time to address. However, treating them as the same concern leads to mismatched protocols and frustrated clients. Options such as the Trexyne Peel are relevant to the pigmentation side of this picture, and understanding the distinction helps practitioners use them at the right time and with the right expectations.
Why the Confusion Between the Two Is So Common
Most clients who have experienced moderate to severe acne will have both conditions simultaneously. An active breakout can cause post-inflammatory hyperpigmentation as it resolves and, if the lesion was deep or the inflammation was severe, leave a textural scar in the same location. When a client presents with uneven, marked skin after acne, they are often looking at a combination of colour changes and textural changes layered on top of each other.
From a distance, or to an untrained eye, the overall impression is simply of damaged, uneven skin. Separating the two components requires a closer clinical assessment and, in some cases, palpation to distinguish whether a mark represents a colour change at the surface or an actual depression or elevation in the skin’s structure.
Getting this assessment right is the foundation of every appropriate treatment plan for post-acne skin. Recommending a resurfacing course to address what a client believes is scarring, only for them to discover the textural issue has not changed, erodes trust even when the pigmentation has genuinely improved.
What Post-Inflammatory Hyperpigmentation Actually Is
Post-inflammatory hyperpigmentation, or PIH, is the flat, discoloured mark that remains after an inflamed acne lesion has healed. It is not a scar in any structural sense. The skin’s surface texture is normal. There is no depression, raised area, or change in the dermis beneath. What has happened is that the inflammatory response generated by the original breakout stimulated melanocytes in the surrounding area to overproduce melanin. That excess melanin deposited unevenly as the lesion healed, leaving a darker patch that can range from light tan to reddish-pink to deep brown depending on the individual’s skin tone and the depth of melanin deposition.
PIH is extremely common in medium, olive, brown, and darker skin tones, reflecting the higher melanocyte activity and stronger inflammatory melanin response in Fitzpatrick skin types III to VI. It can also occur in lighter skin types, where it often presents as pink or red marks rather than brown ones, sometimes referred to as post-inflammatory erythema.
The key clinical point about PIH is that it is a surface and epidermal concern. It involves pigment, not structure. This makes it a viable target for professional resurfacing approaches that support cell turnover and gradually bring pigmented cells to the surface to be replaced with unpigmented ones.
What Acne Scarring Actually Is
Acne scarring is structurally different. When an acne lesion damages the dermis, the skin’s collagen network in that area is disrupted. As the wound heals, the collagen that is laid down to repair the damage may be insufficient, leading to a depression in the skin surface known as an atrophic scar. Alternatively, in some skin types, excess collagen production leads to a raised or hypertrophic scar.
Atrophic acne scars are the most common type and present in several forms. Ice pick scars are narrow, deep, and sharply defined. Rolling scars create a wave-like or undulating texture across broader areas of the skin. Boxcar scars have defined, steep edges and a flat base, creating a pitted appearance. Each of these represents a real structural change in the dermis that resurfacing alone cannot fully correct.
Hypertrophic scars and keloids involve raised, thickened tissue and are less common in acne than atrophic scarring, but they require a different approach to treatment and are outside the scope of standard resurfacing protocols.
Why Depth Determines Treatability
The depth of the original injury determines both the type of scarring that results and how well it responds to any given treatment. Superficial scars that sit closer to the dermal-epidermal junction can show improvement with consistent professional resurfacing over time. Deep, structural scars that extend well into the dermis require more invasive interventions to produce meaningful textural change.
This is why managing client expectations for acne scar treatment requires a thorough assessment of scar depth and type at consultation, not simply an agreement to proceed with resurfacing because the skin looks uneven.
How to Tell Them Apart in a Consultation
The clinical distinction between PIH and acne scarring becomes clearer with a structured assessment approach. The following questions and observations help separate the two:
When stretched gently, does the mark disappear or reduce significantly? A flat colour change will not alter meaningfully when the skin is stretched, but a rolling scar may temporarily flatten when the surrounding skin is pulled taut.
Is the skin texture smooth over the mark, or is there a discernible depression or elevation? Running a clean finger lightly over the area in good lighting can reveal textural changes that are not immediately obvious to the naked eye.
How long ago did the original breakout resolve? PIH that is still recent may appear more intense than it will at its settled baseline, while structural scars do not change in appearance over time.
What is the client’s skin tone and scarring history? Darker skin tones are more prone to PIH. A history of previous significant acne often correlates with a higher likelihood of structural scarring.
The Treatment Relevance of Getting the Diagnosis Right
The reason this distinction matters clinically is that treatment recommendations differ significantly between the two conditions. Post-inflammatory hyperpigmentation is a strong candidate for professional resurfacing because it involves surface and epidermal pigmentation that responds to accelerated cell turnover. A mechanical resurfacing treatment can support the progressive displacement of pigmented cells with fresh, unpigmented ones over a course of sessions.
Acne scarring, particularly moderate to deep atrophic scarring, generally requires treatments that work at a dermal level to stimulate collagen remodelling and structural improvement. Resurfacing can support surface refinement alongside these treatments, but it is not the primary intervention for structural scars.
For clients presenting with a combination of both, which is the most common scenario, a well-considered protocol may use professional resurfacing to address the pigmentation component while a separate or complementary approach is planned for the structural scarring, based on the severity and type of scars present.
Where the Trexyne Peel Fits Into Post-Acne Skin Treatment
The Trexyne Peel is a mechanical resurfacing treatment built around marine-algae spicules that create controlled micro-channels in the skin’s surface without any chemical exfoliants involved. This makes it a considered option for addressing the post-inflammatory hyperpigmentation component of post-acne skin, supporting cell turnover and skin renewal in a way that avoids the chemical inflammatory response that acid-based resurfacing can generate.
For skin that is already sensitised from a history of acne and previous treatments, the mechanical mechanism is clinically relevant. PIH-prone skin benefits from resurfacing that encourages renewal without adding further inflammatory stimulus that could restimulate melanocyte activity. Stabilised Vitamin E in the formulation supports the recovery phase from the first application, helping to manage post-treatment repair efficiently in skin that may have a compromised barrier from years of acne-related inflammation.
Managing Both Concerns Within a Coherent Protocol
Clients who present with both PIH and structural acne scarring need a clear, staged treatment plan that addresses each component with an appropriate approach. Attempting to address everything simultaneously with a single treatment type often produces suboptimal results for both concerns.
A structured approach might prioritise barrier restoration and PIH management first, using a course of professional mechanical resurfacing to address the pigmentation and support overall skin health before introducing treatments targeted at structural scarring. This sequencing makes practical sense because a skin in better overall condition, with a restored barrier and reduced inflammatory baseline, will generally respond better to any subsequent intervention.
The tiered protocol within the Trexyne Peel framework gives practitioners the flexibility to adjust intensity across a treatment course based on the skin’s response and condition at each appointment. For post-acne skin that can vary considerably in how it presents from session to session, this adjustability is a genuine clinical advantage.
Practitioners interested in exploring professional botanical resurfacing for post-acne skin can browse the full range via the Trexyne shop, or speak directly with the team through the Trexyne contact page.
Setting Accurate Expectations With Clients
Clients dealing with the aftermath of acne often carry significant distress about how their skin looks and may have unrealistic expectations about how quickly it can be corrected. Setting accurate, compassionate expectations at consultation is one of the most important things a practitioner can do for this client group.
The key messages to communicate clearly are that PIH can improve meaningfully with the right professional treatment course, that structural scarring requires a different and often more extended treatment pathway, that both conditions improve more slowly than clients typically expect, and that consistent SPF use throughout any treatment course is essential to prevent new pigmentation developing alongside the marks being treated.
Clients who understand the distinction between what the resurfacing treatment is addressing and what it is not are far better positioned to evaluate their results accurately and to commit to the longer-term protocol that post-acne skin genuinely requires.
Further information on Trexyne’s approach to professional botanical resurfacing is available on the Trexyne website.
Conclusion
Acne dark marks and acne scarring are different conditions that require different treatment strategies. Post-inflammatory hyperpigmentation is a pigmentation change driven by the inflammatory response to acne, sitting within the skin’s surface layers and responding progressively to professional resurfacing. Acne scarring involves structural changes to the dermis where collagen has been disrupted, requiring approaches that address the skin at a deeper level. The two often coexist in the same client, and distinguishing between them accurately at consultation is the foundation of a treatment plan that sets appropriate expectations and delivers genuine results. For the pigmentation component of post-acne skin, the Trexyne Peel offers a mechanical resurfacing approach without chemical exfoliants, stabilised Vitamin E to support recovery, and a tiered protocol that adapts to variable post-acne skin conditions. Used consistently and alongside appropriate photoprotection, it may support a visible improvement in post-inflammatory hyperpigmentation and contribute to a more even-looking complexion over the course of a well-managed treatment plan.
FAQs
Q: What is the difference between acne scarring and acne dark marks?
Acne dark marks, known as post-inflammatory hyperpigmentation, are flat discolourations caused by excess melanin production following an inflamed breakout. They involve no structural change to the skin. Acne scarring involves actual damage to the dermis, where disrupted collagen creates depressions or raised areas in the skin’s surface. Both can appear after acne, but they require different treatment approaches.
Q: Can the Trexyne Peel help with acne dark marks?
The Trexyne Peel supports skin renewal through a mechanical resurfacing mechanism that encourages cell turnover, which can contribute to the gradual fading of post-inflammatory hyperpigmentation over a course of professional treatments. It resurfaces through marine-algae spicules with no acids involved, making it a considered option for sensitised post-acne skin that needs a gentler resurfacing approach.
Q: Will resurfacing treatments improve acne scars?
Resurfacing treatments can contribute to surface refinement and may support modest improvements in superficial scarring over time, but they are not the primary treatment for structural acne scars, particularly moderate to deep atrophic scars. A practitioner assessment of scar type and depth is essential before making treatment recommendations for structural scarring.
Q: How long does post-inflammatory hyperpigmentation from acne last?
PIH can persist for months or years without professional intervention, particularly in medium to darker skin tones where melanin responses to inflammation tend to be stronger. The timeline depends on the depth of melanin deposition, how consistently daily SPF is used, and whether a professional resurfacing course is supporting the skin’s renewal process.
Q: Why do darker skin tones get more pronounced dark marks after acne?
Darker skin tones have higher baseline melanocyte activity, which means the melanin response to inflammation tends to be stronger. When acne triggers that inflammatory response, melanocytes are more likely to produce significant excess melanin in the affected area, leading to more visible and longer-lasting post-inflammatory hyperpigmentation.
Q: Is it safe to have a professional peel if I still have active acne?
Resurfacing treatments should not be applied to actively inflamed or broken-out skin. A professional treatment course for post-inflammatory hyperpigmentation is best planned for periods when breakout activity is low or absent. A practitioner assessment at each appointment will determine whether the skin is in a suitable state to proceed at any given session.
Q: Where can I find out more about using the Trexyne Peel for post-acne pigmentation?
Practitioners can explore the full Trexyne product range via the Trexyne shop, or contact the team directly through the Trexyne contact page for further information on incorporating professional botanical resurfacing into post-acne treatment protocols.