What Is Melasma and How Is It Different From Pigmentation?
Melasma is a specific type of pigmentation driven primarily by hormonal factors rather than UV damage alone, and understanding this distinction matters enormously when it comes to treatment. The word “pigmentation” is a broad term covering any form of uneven skin colour, including age spots, post-inflammatory dark marks, and freckles. Melasma is one type within that category, but it has a particular set of characteristics, triggers, and treatment sensitivities that set it apart from other pigmentation concerns. Getting the diagnosis right before any resurfacing treatment begins is not optional. Treating melasma as if it were straightforward sun damage, or applying an approach that works well for post-inflammatory hyperpigmentation to a melasma presentation, often produces disappointing results or actively worsens the condition. For practitioners using mechanical resurfacing options such as the Trexyne Peel, understanding where melasma fits within the wider pigmentation picture is essential clinical context.
What Melasma Actually Is
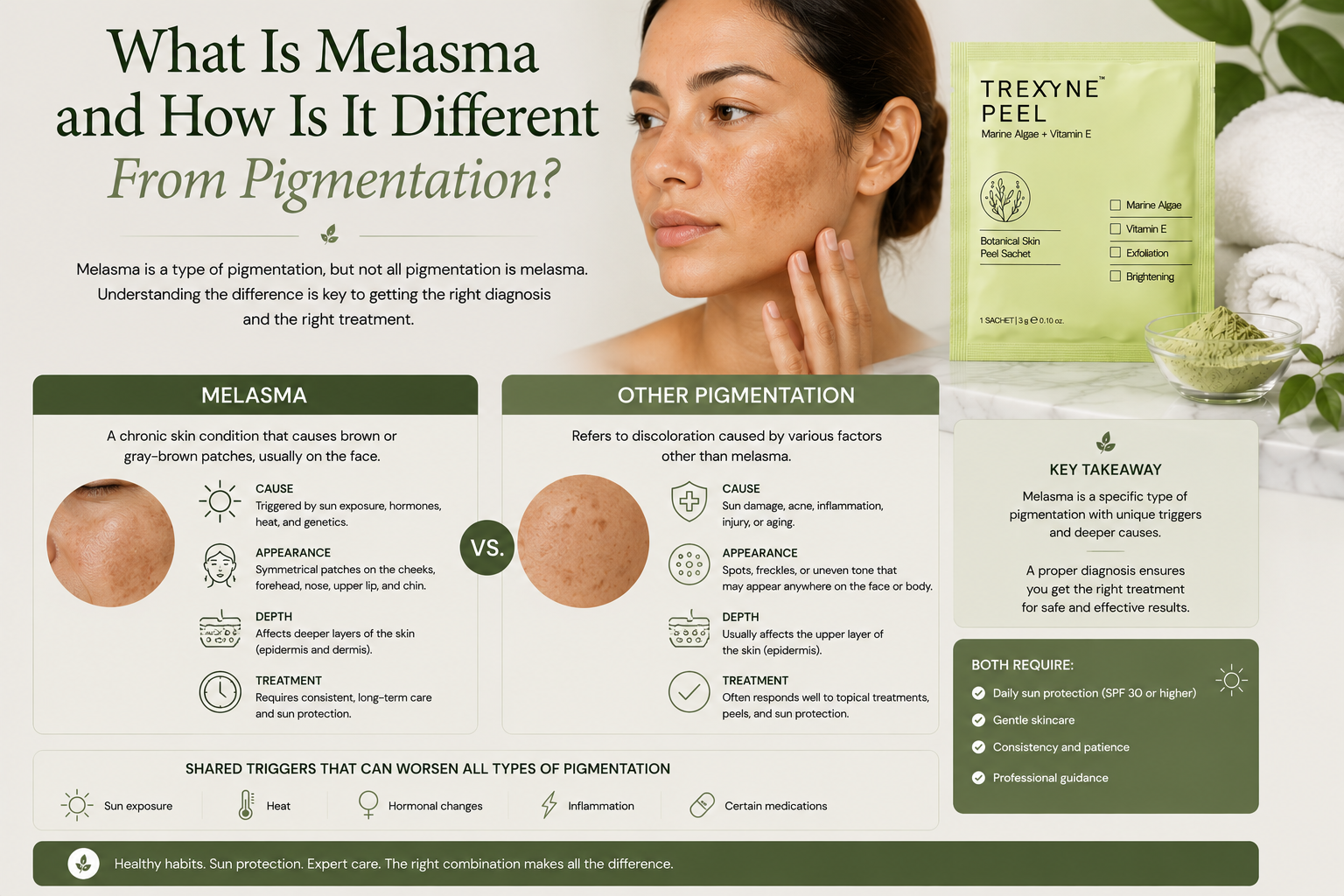
Melasma is a chronic acquired pigmentation disorder characterised by symmetrical, irregular patches of brown to grey-brown discolouration. It appears most commonly across the cheeks, forehead, upper lip, and bridge of the nose, following a distribution that broadly mirrors the pattern of areas most influenced by hormonal activity and UV exposure simultaneously.
The condition develops when melanocytes, the cells responsible for producing melanin, become chronically overactive in specific areas of the face. Unlike the localised, defined deposits of age spots or the post-inflammatory response that produces dark marks after a breakout, melasma involves a diffuse, persistent elevation in melanocyte activity that can be difficult to resolve completely because the underlying hormonal and environmental triggers often remain active even during treatment.
It is significantly more common in women than men, particularly those with medium to darker skin tones in Fitzpatrick types III to VI, though it can occur across all skin types. Geographical distribution suggests higher prevalence in populations with more intense year-round UV exposure, though the condition is widely seen across the UK, particularly in clients with hormonal risk factors.
The Hormonal Trigger That Makes Melasma Distinctive
The most important clinical distinction between melasma and other forms of hyperpigmentation is the hormonal component. Melasma is strongly associated with elevated oestrogen and progesterone levels, which is why it so frequently develops during pregnancy, when using hormonal contraception, or around the menopause when hormonal fluctuations are significant.
Hormonal changes do not directly produce the pigmentation. They work indirectly by increasing melanocyte sensitivity to UV radiation and other triggers. Melanocytes in hormonally primed skin produce more melanin in response to the same UV stimulus that would produce a less significant response in skin without that hormonal influence. This is why melasma characteristically worsens during the summer months and improves, though rarely resolves entirely, when UV exposure reduces in winter.
This hormonal mechanism is why melasma is so much harder to treat than sun-induced pigmentation. For age spots, the trigger, cumulative UV, can be substantially controlled by consistent sun protection, which allows resurfacing to make clear, sustained progress. For melasma, the hormonal trigger may remain active throughout and even beyond a treatment course, meaning the melanocytes are continuing to receive a signal to produce excess pigment even as resurfacing attempts to displace the resulting deposits.
How Melasma Differs From Age Spots
Age spots and melasma are both forms of hyperpigmentation involving excess melanin, but they differ in their cause, their appearance, their distribution, and their response to treatment.
Age spots develop from the direct cumulative effect of UV radiation on specific areas of the skin, producing localised, defined deposits of melanin that do not change significantly between summer and winter once established. They tend to present as clearly defined, flat spots with relatively consistent colour within each lesion, and they appear most commonly on the face, hands, and forearms in areas with the highest lifetime UV exposure.
Melasma presents as broader, more diffuse patches with irregular, feathered borders. The colour within a patch can be variable, shifting between brown and grey tones. Melasma is typically bilateral, appearing on both sides of the face in a broadly symmetrical pattern, which is one of the diagnostic clues that distinguishes it from isolated sun-induced spots. Unlike age spots, melasma can fluctuate visibly with the seasons, hormonal cycle, and UV exposure, appearing to darken or improve over relatively short time periods.
Understanding these visual differences helps practitioners make a more accurate assessment at consultation, which is the foundation of any appropriate treatment plan.
How Melasma Differs From Post-Inflammatory Hyperpigmentation
Post-inflammatory hyperpigmentation, or PIH, is the dark discolouration that follows an inflammatory event in the skin, such as an acne breakout, skin injury, or a treatment that provoked an excessive inflammatory response. It tends to appear in the exact area and shape of the original inflammation, making it relatively straightforward to identify when the client can recall the triggering event.
Melasma does not follow a specific area of inflammation or injury. It develops in response to hormonal signals and UV exposure rather than a discrete inflammatory event. This means there is no single “cause” to point to in the way there is with PIH, which makes patient education around melasma more complex.
The two conditions can coexist in the same client. A client with a hormonal melasma pattern may also develop PIH after a breakout or a treatment reaction, and distinguishing which dark patches belong to which category requires careful clinical assessment rather than a general assumption that all pigmentation in a client with known melasma is hormonally driven.
Why Melasma Responds Differently to Resurfacing
Because melasma is hormonally influenced and often sits in both the epidermal and dermal layers of the skin, it requires a more cautious and carefully managed resurfacing approach than other pigmentation types. Several factors make it particularly challenging.
The inflammatory trigger risk is higher. Melasma-prone skin is more likely to respond to inflammatory stimulus with additional melanin production. This means resurfacing treatments that generate a significant chemical inflammatory response can worsen melasma rather than improving it, even when the same treatment would be effective for age spots or PIH in a different client.
The active hormonal trigger may remain throughout treatment. Unlike sun damage, which can be substantially controlled by consistent SPF use, hormonal influences on melanocyte activity are internal and cannot be fully neutralised by topical measures. This means progress from resurfacing can be partially counteracted by ongoing hormonal melanocyte stimulation, producing a slower and less predictable response than practitioners might see with other pigmentation types.
Dermal melasma, where pigment has been deposited in the deeper dermal layer rather than the superficial epidermis, does not respond to resurfacing at all, since resurfacing works by stimulating renewal in the epidermis rather than the dermis. Identifying whether a client’s melasma is epidermal, dermal, or mixed before committing to a resurfacing course is part of a thorough assessment.
Where the Trexyne Peel Fits in Managing Melasma
The Trexyne Peel resurfaces through marine-algae spicules via a mechanical mechanism, with no chemical exfoliants involved at any stage. For melasma clients, the absence of a chemical inflammatory trigger is clinically relevant. Because the treatment does not generate the chemical inflammatory response associated with acid-based peels, it reduces the risk of restimulating the melanocyte pathway that can worsen melasma during and after treatment.
Stabilised Vitamin E in the formulation supports the skin’s recovery phase from the first application, which matters for melasma clients where the recovery period can be a window of particular vulnerability to inflammatory triggers. The tiered protocol allows the practitioner to begin conservatively and progress only as the skin demonstrates its tolerance, which is the appropriate approach for a skin type that needs careful management throughout the course.
Melasma management through resurfacing is a slow, gradual process and practitioners should communicate this clearly before any course begins. Visible improvement in melasma requires patience, consistent SPF use throughout, and an honest understanding that the condition may be managed and improved rather than fully resolved, particularly while hormonal triggers remain active.
The Essential Role of Sun Protection in Melasma Management
For any pigmentation concern, daily broad-spectrum SPF is important. For melasma specifically, it is indispensable. UV exposure is the most powerful amplifier of melasma activity, and without consistent, rigorous sun protection, no resurfacing approach can produce sustainable results because the melanocytes are continuously restimulated between sessions.
Clients with melasma should apply broad-spectrum SPF every morning as a non-negotiable step, reapply when outdoors for extended periods, and use additional physical protection such as hats and shade during peak UV hours. These measures do not treat existing melasma, but they substantially limit the rate at which the condition progresses and protect the improvement achieved through professional resurfacing.
Practitioners looking to incorporate mechanical resurfacing into their melasma management protocols can explore the full product range via the Trexyne shop, or contact the team directly through the Trexyne contact page.
When to Refer a Melasma Client to a Dermatologist
Not all melasma cases are appropriate for management within the aesthetic clinic setting, and recognising when onward referral is needed is part of good clinical practice. Clients with very extensive or severe melasma, with a significant dermal component, or with a history of treatment that has consistently failed or worsened the condition may benefit from dermatological assessment before any further aesthetic intervention is planned.
Clients on hormonal medications that may be driving the melasma should discuss whether any adjustment to those medications is appropriate with their prescribing doctor. This is not a conversation the aesthetic practitioner should have on behalf of the GP or prescriber, but raising it as a relevant factor in the overall management picture is appropriate.
More information on the Trexyne approach to professional botanical resurfacing is available on the Trexyne website.
Conclusion
Melasma is a distinct form of hyperpigmentation driven by hormonal factors and UV exposure, characterised by symmetrical, diffuse patches across the central face that differ from age spots and post-inflammatory pigmentation in their cause, appearance, and response to treatment. Unlike other pigmentation concerns, melasma involves melanocytes that may remain continuously stimulated by an active hormonal trigger, making it slower to respond to resurfacing and more likely to return if sun protection is not rigorous. Treating it requires a resurfacing approach that minimises the risk of inflammatory restimulation and is applied with patience and conservative progression. The Trexyne Peel offers a mechanical resurfacing mechanism with no chemical exfoliants, stabilised Vitamin E to support recovery, and a tiered protocol suited to the careful management that melasma requires. Used consistently alongside daily sun protection and honest expectation-setting, it may support visible improvement in melasma as part of a well-managed professional treatment plan.
FAQs
Q: What is melasma and how is it different from other pigmentation?
Melasma is a hormonally influenced pigmentation condition characterised by symmetrical, diffuse brown to grey-brown patches, most commonly across the cheeks, forehead, and upper lip. It differs from other pigmentation types such as age spots and post-inflammatory hyperpigmentation in its hormonal cause, its bilateral distribution, and its tendency to fluctuate with UV exposure and hormonal changes rather than remaining stable.
Q: What causes melasma to develop?
Melasma develops when hormonal changes, particularly elevated oestrogen and progesterone, increase melanocyte sensitivity to UV radiation. This is why it commonly appears during pregnancy, with hormonal contraception, or around the menopause. UV exposure acts as the primary trigger that converts this heightened sensitivity into visible pigmentation, which is why melasma typically worsens in summer and improves in winter.
Q: Why is melasma harder to treat than age spots?
Melasma involves an active hormonal trigger that may remain present throughout and after a treatment course, meaning melanocytes continue to receive a signal to produce excess pigment even as resurfacing attempts to displace existing deposits. Age spots are driven by cumulative UV damage that can be substantially controlled by consistent sun protection, allowing resurfacing to make clearer, more sustained progress.
Q: Can the Trexyne Peel help with melasma?
The Trexyne Peel’s mechanical mechanism avoids the chemical inflammatory trigger that can worsen melasma in susceptible skin, and its tiered protocol allows conservative progression suited to the careful management melasma requires. Visible improvement in melasma from resurfacing is gradual, and daily broad-spectrum SPF use throughout and after the course is essential to support results.
Q: Does melasma ever go away on its own?
Melasma can fade during periods of lower hormonal activity or reduced UV exposure, such as post-pregnancy or during winter months. However, it rarely resolves fully without professional intervention, particularly in clients with a long history of the condition or a persistent hormonal trigger. Even after successful treatment, it can return with UV exposure or hormonal changes if sun protection is not maintained.
Q: Is melasma the same as the mask of pregnancy?
Yes. The mask of pregnancy, clinically known as chloasma, is the term for melasma that appears during pregnancy. It is the same condition, driven by the elevated oestrogen and progesterone levels of pregnancy sensitising melanocytes to UV stimulus. It may fade after delivery as hormonal levels normalise, but it can persist and often requires professional management to resolve fully.
Q: How important is SPF for managing melasma?
Daily broad-spectrum SPF use is the single most important step in managing melasma, both during a professional treatment course and long-term. UV exposure continuously stimulates the hormonally primed melanocytes responsible for melasma, and without rigorous sun protection, no resurfacing treatment can produce sustainable improvement. SPF should be applied every morning and reapplied when outdoors, regardless of season.