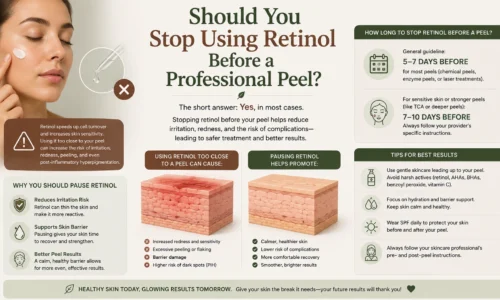
What Causes Pigmentation on the Face?
Facial pigmentation is one of the most searched-for skin concerns worldwide, and for good reason. The face is exposed to more environmental triggers than almost any other part of the body, and it is where changes in skin tone are most immediately visible. Pigmentation on the face develops when the skin overproduces a pigment called melanin in specific areas, resulting in dark spots, patches, and an uneven complexion. Several triggers cause this to happen, and understanding them is the key to finding a treatment that actually works. For those who have tried topical products without success, a professional solution like the Trexyne Peel offers a more targeted approach to reducing facial pigmentation and restoring a clearer skin tone.
Why the Face Is Particularly Prone to Pigmentation
The skin on the face is uniquely vulnerable to pigmentation for several reasons. It receives more daily UV exposure than almost any other area of the body. It is also thinner and more sensitive than skin elsewhere, which means it responds more visibly to hormonal shifts, inflammation, and environmental stressors.
The face also has a higher density of sebaceous glands and is more frequently affected by acne, making it a prime site for post-inflammatory pigmentation. When you combine that with years of sun exposure and the hormonal fluctuations that many people experience throughout their lives, it becomes clear why facial pigmentation is so common and so persistent.
The melanocytes in facial skin respond quickly to stimulation, which is useful as a form of UV protection but problematic when it results in lasting discoloration that does not fade on its own.
1. Sun Exposure and UV Damage
Ultraviolet radiation from the sun is the leading cause of pigmentation on the face. Every time the skin is exposed to UV light without protection, melanocytes receive a signal to produce more melanin. In the moment, this appears as a tan or a slightly deeper tone. Over months and years of repeated exposure, it accumulates as concentrated dark patches and sunspots that do not fade when the tan does.
The cheeks, nose, forehead, and upper lip are particularly affected because they are the most consistently sun-exposed zones on the face. People who spend time outdoors regularly, even in everyday activities like commuting or walking, are accumulating UV exposure that adds up over time.
UV damage is cumulative. The pigmentation you see on your face at 40 or 50 often reflects sun exposure that occurred over decades, not just recently. This is why consistent daily sunscreen use is considered the most important single step in both preventing new facial pigmentation and protecting the results of any treatment.
2. Hormonal Changes
Hormones have a direct influence on melanocyte activity in the skin. Estrogen and progesterone can stimulate melanocytes to produce excess melanin, which is why significant hormonal events often cause visible changes in facial skin tone.
The most well-known hormonally driven pigmentation condition is melasma. It appears as large, symmetrical patches of brown or gray-brown discoloration across the forehead, cheeks, upper lip, and bridge of the nose. The pattern is often described as a mask-like appearance, which is why melasma is sometimes called the mask of pregnancy.
Pregnancy is the most common hormonal trigger, but oral contraceptives, hormonal intrauterine devices, and hormone replacement therapy can all cause or worsen melasma. Because the hormonal trigger may remain active for an extended period, melasma is one of the more challenging types of facial pigmentation to treat and is prone to returning after treatment if sun protection and hormonal management are not maintained.
3. Acne and Post-Inflammatory Hyperpigmentation
Acne is one of the most common causes of facial pigmentation, and it affects people across a wide age range. When a pimple becomes inflamed, the skin launches a healing response that includes activation of melanocytes in and around the affected area. These cells produce melanin as part of the repair process, and once the pimple heals, the excess pigment remains as a flat dark mark.
This is called post-inflammatory hyperpigmentation, and it is particularly common in people with medium to dark skin tones, whose melanocytes are inherently more reactive to inflammation. Even relatively minor breakouts can leave marks that persist for months.
Picking or squeezing pimples significantly increases the risk of post-inflammatory pigmentation because it deepens the inflammation and introduces additional trauma to the skin. The same applies to using abrasive scrubs or harsh products on actively inflamed skin.
Beyond acne, other inflammatory conditions such as eczema, seborrheic dermatitis, and allergic reactions can also trigger post-inflammatory hyperpigmentation on the face when they occur repeatedly or are poorly managed.
4. Aging and Cumulative Sun Damage
As the skin ages, the mechanisms that regulate melanin production become less precise. Melanocytes may become unevenly distributed across the skin, and the enzyme systems that control pigment synthesis lose their accuracy. Combined with decades of accumulated UV exposure, this leads to the age spots and general patchiness that become more visible from the mid-thirties onward.
Cell turnover also slows significantly with age. In younger skin, the surface layer renews itself every three to four weeks. In older skin, this cycle extends to six weeks or longer. Pigmented cells stay on the surface for longer, which makes existing spots appear more pronounced and slows the natural fading process.
The result is a face that shows years of environmental exposure through its uneven tone, concentrated spots, and loss of the bright, even quality that characterizes younger skin. While aging itself cannot be reversed, treating the effects of cumulative damage is entirely achievable with the right professional approach.
5. Medications That Cause Facial Pigmentation
Certain medications can trigger or worsen facial pigmentation as a side effect. Some increase the skin’s sensitivity to UV light, a property called photosensitivity, meaning that even brief sun exposure can trigger a disproportionate melanin response. Others interfere directly with melanin metabolism.
Medications commonly associated with facial pigmentation include:
- Tetracycline-based antibiotics, often prescribed for acne
- Oral contraceptives and hormone-based medications
- Antimalarial drugs such as hydroxychloroquine
- Nonsteroidal anti-inflammatory drugs taken long term
- Some antiepileptic medications
- Certain chemotherapy agents
If you notice new or worsening facial pigmentation after starting a medication, it is worth raising this with your prescribing doctor. In some cases, an alternative can be considered, or stricter sun protection measures can be put in place to minimize the skin’s response.
6. Friction, Heat, and Repeated Physical Irritation
Repeated physical irritation to the face can trigger pigmentation in a similar way to inflammation from acne. Rubbing the skin vigorously, using rough towels, wearing tight headwear that presses against the forehead, or regularly touching the face all introduce minor trauma that the skin’s melanocytes respond to over time.
Heat-induced pigmentation is another underrecognized trigger. Regular exposure to intense heat sources, whether from professional environments, cooking, or saunas, can stimulate melanin production in the skin without UV radiation being involved. This is sometimes called erythema ab igne, or heat-induced pigmentation, and it appears as a mottled, net-like discoloration on the affected area.
Modifying the habits that cause repeated irritation is an important part of preventing new facial pigmentation from forming, alongside any treatment used to address what is already there.
7. Genetics and Skin Type
Your genetic background plays a meaningful role in how prone your skin is to developing facial pigmentation. People with certain ethnicities, particularly those of South Asian, East Asian, Middle Eastern, Latin American, and African descent, tend to have more reactive melanocytes and are statistically more likely to develop hyperpigmentation in response to the triggers described above.
Fitzpatrick skin types IV through VI, which encompass medium-brown to deep complexions, show a higher incidence of post-inflammatory hyperpigmentation and melasma. While this reflects a biological reality, it does not mean that treatment is less achievable. It does mean that treatment must be more carefully calibrated to avoid causing additional irritation that could worsen the pigmentation.
A family history of melasma or persistent dark spots is also a reliable predictor of personal susceptibility, and it reinforces the importance of early preventive habits like consistent SPF use.
Why Facial Pigmentation Is Hard to Treat Without Professional Help
Many people spend months using brightening serums and spot treatments only to find that their facial pigmentation remains essentially unchanged. This is not simply a matter of patience. There are structural reasons why topical products struggle to produce meaningful results for established pigmentation.
Melanin can accumulate in both the superficial epidermis and deeper layers. Over-the-counter products are formulated for safety at low concentrations, which limits how deeply their active ingredients can penetrate. They may slow new melanin production modestly but rarely reach the established deposits that have built up over time.
Professional treatments address this limitation by working at a deeper level. A professional pigmentation treatment like the Trexyne Peel uses higher-concentration actives applied under clinical supervision to physically remove layers of pigmented skin and stimulate the skin’s renewal process. This is a fundamentally more direct approach that produces measurable results where topical products have stalled.
How Trexyne Peel Targets Facial Pigmentation
The Trexyne Peel is a professionally administered chemical peel formulated to address the specific challenges of facial pigmentation. Applied by a trained skincare practitioner, it uses controlled chemical exfoliation to loosen and remove the outer layers of the skin where excess melanin is concentrated.
Each session works to clear a layer of pigmented surface skin, revealing fresher, more evenly toned cells beneath. At the same time, it signals the deeper skin layers to produce new cells at an accelerated rate, which shortens the time it takes for the surface to renew. With a properly structured series of treatments and consistent sun protection between sessions, patients see a progressive reduction in dark spots, a more uniform skin tone, and improved overall clarity.
The treatment is customized by the practitioner based on skin type, pigmentation type, and the degree of discoloration present, which means it can be safely adapted for a range of skin tones and concerns rather than taking a one-size-fits-all approach.
Conclusion
Facial pigmentation develops through a combination of triggers, including UV exposure, hormonal shifts, acne, aging, medication, physical irritation, and genetic predisposition. The face is uniquely vulnerable because it is exposed to nearly all of these factors simultaneously and repeatedly over the course of a lifetime.
Effective treatment begins with understanding which triggers are active in your own case and addressing them alongside professional intervention. For those ready to see real progress with their facial pigmentation, advanced skin peel solutions such as the Trexyne Peel provide a clinically grounded path to a clearer, more even, and more confident complexion.
Frequently Asked Questions
1. What causes pigmentation on the face specifically?
Facial pigmentation is most commonly caused by UV exposure from sunlight, which triggers excess melanin production in sun-exposed areas. Hormonal changes from pregnancy, contraceptives, or hormonal therapy can cause melasma, a specific type of facial pigmentation. Acne and skin inflammation leave post-inflammatory dark marks. Aging, certain medications, and genetics also contribute, often working together to create or worsen visible discoloration on the face.
2. Why is facial pigmentation more visible than pigmentation on other parts of the body?
The face receives more daily UV exposure than most other body areas, has thinner and more reactive skin, and is more frequently affected by acne and hormonal fluctuations. All of these factors combine to make the face more susceptible to developing visible pigmentation. The face is also the most observed area of the body, which means even minor discoloration is noticed more readily than it would be elsewhere.
3. Can acne cause permanent pigmentation on the face?
Acne itself does not cause permanent scarring in every case, but the post-inflammatory hyperpigmentation it leaves behind can persist for a very long time without treatment, sometimes for a year or more. This type of pigmentation is not truly permanent in most cases, but it does require active treatment and consistent sun protection to fade meaningfully. Professional options like the Trexyne Peel can significantly speed up this process.
4. Does stress make facial pigmentation worse?
Stress can worsen facial pigmentation indirectly. Chronic stress triggers hormonal changes, including elevated cortisol, that can influence melanocyte activity. It also tends to aggravate inflammatory skin conditions like acne and eczema, which in turn increase the risk of post-inflammatory pigmentation. Managing stress is a meaningful, if indirect, part of an overall approach to skin health.
5. What is the fastest way to treat facial pigmentation?
Professional treatments produce faster and more significant results than topical products alone. A series of Trexyne Peel sessions removes pigmented surface cells and accelerates skin renewal, producing visible improvement in weeks rather than months. Combining professional treatment with daily broad-spectrum sunscreen and a targeted home routine gives the best chance of achieving rapid, lasting results.
6. Why does melasma on the face keep coming back?
Melasma recurs because its primary triggers, hormonal activity and UV exposure, are often ongoing. Even after successful treatment, if the hormonal stimulus remains active and sun protection is not maintained consistently, the melanocytes will produce new pigmentation. Managing melasma is typically an ongoing process of treatment and maintenance rather than a one-time fix, which is why working with a knowledgeable practitioner is important.
7. Is the Trexyne Peel suitable for treating pigmentation on all facial skin tones?
Trexyne Peel can be adapted for a range of skin tones, but the approach needs to be carefully calibrated for darker complexions, which are more sensitive to over-stimulation that could worsen pigmentation. A qualified practitioner with experience treating diverse skin types will assess your specific situation before proceeding and will customize the treatment to minimize risk while maximizing results. This is one reason choosing an experienced provider is essential.