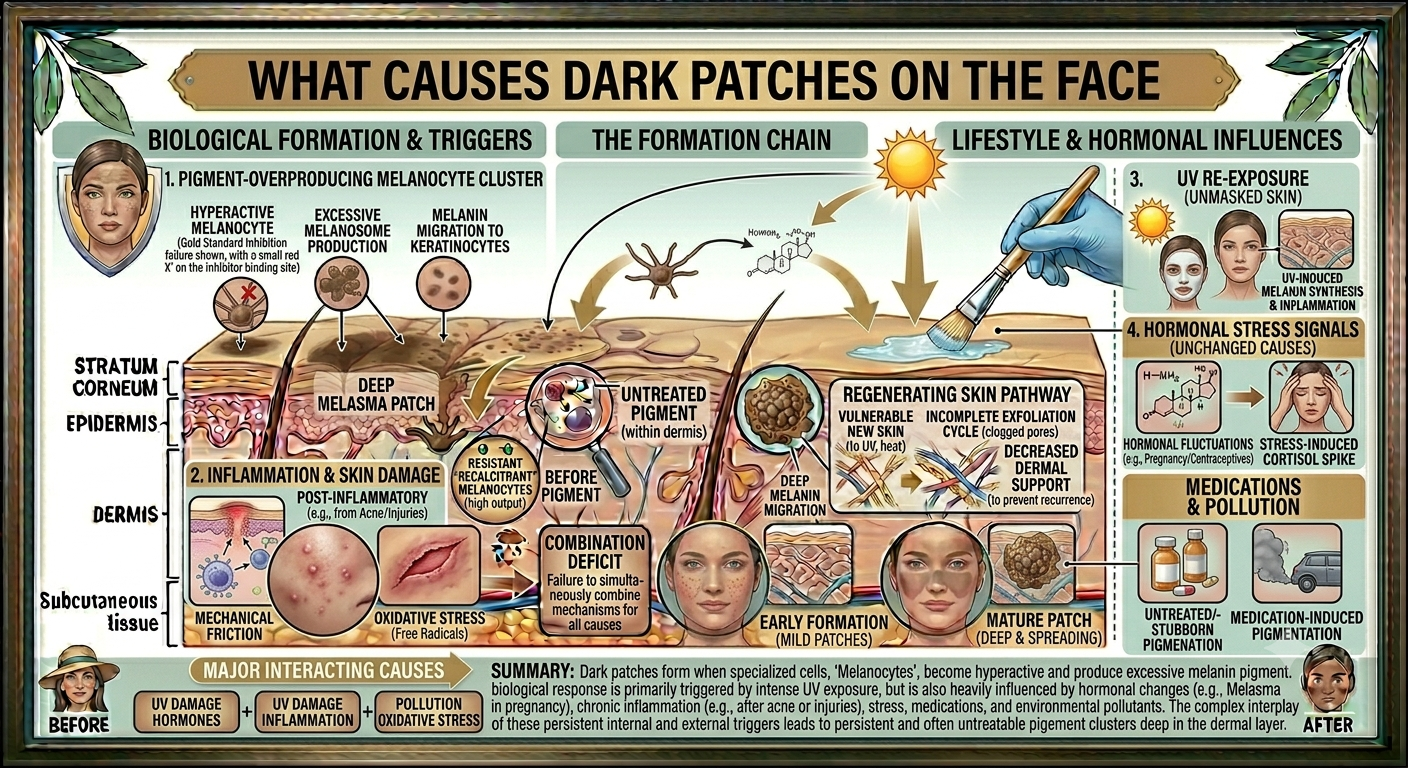
What Causes Dark Patches on the Face
Dark patches on the face develop when melanocytes — the cells responsible for producing skin pigment — become overactive in a specific area. The result is an uneven distribution of melanin that shows up as patches darker than the surrounding skin. The causes range from UV exposure and inflammation through to hormonal changes and certain medications. Identifying the cause matters because it shapes the treatment plan. Resurfacing alone is rarely enough without understanding what triggered the pigmentation in the first place. For practitioners building a targeted approach to facial hyperpigmentation, the Trexyne Peel — Professional Algae Resurfacing Treatment offers a botanical, mechanical resurfacing option that may support skin renewal as part of a wider management strategy.
How Pigmentation Actually Forms
Understanding pigmentation at a cellular level makes it easier to explain to clients and to choose the right treatment approach. Melanin is produced by melanocytes in the basal layer of the epidermis. Under normal conditions, melanin distributes evenly and gives the skin its baseline colour. When something triggers an exaggerated response in a localised area, excess melanin accumulates and a patch forms.
The skin’s natural cell turnover cycle should, in theory, gradually clear surface pigmentation as cells migrate upward and shed. The problem arises when turnover slows, when the melanocytes keep producing at a faster rate than shedding can clear, or when the pigment has penetrated deeper into the dermis where it becomes far more resistant to surface treatment.
Epidermal vs. Dermal Pigmentation
Not all dark patches sit at the same depth. Epidermal pigmentation sits in the upper layers of the skin and tends to respond better to resurfacing treatments. Dermal pigmentation sits deeper and is harder to address with surface-level approaches alone. Mixed pigmentation involves both layers and requires the most considered management. Identifying the likely depth of the pigmentation during consultation helps set realistic treatment expectations.
Sun Exposure and UV Damage
UV radiation is the most well-documented trigger for facial dark patches. Both UVA and UVB rays stimulate melanocyte activity as a protective response. Over time, repeated exposure leads to cumulative pigmentation that manifests as solar lentigines — the flat, well-defined spots commonly called sun spots or age spots.
These tend to cluster where UV exposure is highest: the cheeks, nose, forehead, and upper lip. They deepen gradually, which is why many clients notice them becoming more prominent in their thirties and forties even if the cumulative UV exposure happened over the preceding decades.
Why SPF Is the Foundation of Any Treatment Plan
No resurfacing programme for UV-induced pigmentation will hold its results without consistent sun protection. UV exposure can re-stimulate the same melanocytes within days of treatment. Clients need SPF 30 as a daily minimum, SPF 50 during summer or with significant outdoor time, and reapplication through the day in high-exposure conditions. This is not supplementary advice. It is a clinical requirement that determines whether treatment produces lasting improvement.
Hormonal Changes and Melasma
Hormonal fluctuations are strongly associated with a specific type of facial dark patches known as melasma. It typically presents as symmetrical, diffuse patches across the cheeks, upper lip, forehead, and bridge of the nose. The distribution pattern is often described as mask-like.
Elevated oestrogen levels are the primary hormonal driver. This is why melasma is particularly prevalent during pregnancy, when it is sometimes called the “mask of pregnancy,” and why it often develops or worsens in clients using hormonal contraception or undergoing hormone replacement therapy. It can also flare in line with natural hormonal cycles.
Why Melasma Behaves Differently From Other Dark Patches
Melasma tends to have both epidermal and dermal components, which makes it more resistant to surface resurfacing alone. It also has a strong recurrence tendency. Even when visible improvement is achieved through treatment, the underlying hormonal drivers remain active. UV exposure can then re-trigger the pigmentation rapidly. Managing melasma requires a longer-term strategy that combines professional treatment with strict sun protection and, where appropriate, a conversation about hormonal contributors.
Post-Inflammatory Hyperpigmentation
Post-inflammatory hyperpigmentation, or PIH, develops after skin trauma. Anything that triggers a localised inflammatory response can leave pigmentation behind: acne breakouts, minor cuts or abrasions, waxing, overly aggressive facial treatments, or even reactions to skincare products. The skin produces excess melanin as part of its protective response to the inflammation, and that pigment remains after the initial event has resolved.
PIH tends to sit in the upper layers of the skin, which makes it more accessible to resurfacing treatments. However, in clients with medium to deeper skin tones, the melanocyte response to inflammation is often more pronounced, meaning PIH can be deeper, more intense, and more likely to recur with any subsequent inflammatory event.
Acne and Persistent Facial Patches
For clients with active or recurrent acne, PIH is a cycle rather than a one-off event. Each new breakout creates the conditions for new post-inflammatory pigmentation. Treating the PIH without managing the acne means that new patches keep forming at roughly the same rate as old ones are clearing. A joined-up approach to both the acne and the resulting pigmentation is essential for this client group.
Medication-Induced Hyperpigmentation
Certain medications can trigger or worsen facial hyperpigmentation as a side effect. Antimalarial drugs, some antibiotics, non-steroidal anti-inflammatory drugs, and certain antipsychotic medications are among those associated with pigmentation changes. Hormonal medications, as discussed above, fall into this category too.
If a client presents with dark patches that began or intensified after starting a new medication, this is worth exploring during the consultation. It does not necessarily mean the medication needs to be changed, but it does affect the treatment approach and expectation-setting. Improvement may be slower or more limited while the medication remains in use.
Age and Slowing Cell Turnover
As we get older, the skin’s natural cell turnover cycle slows down. In younger skin, surface pigmentation sheds relatively efficiently as part of the renewal cycle. In older skin, cells spend longer at the surface, which means pigment accumulates more visibly and fades more slowly. This is one of the reasons dark patches become more common and more persistent from the mid-thirties onward.
This is also where professional resurfacing becomes particularly relevant. By creating a stimulus for cell renewal, resurfacing treatments can help compensate for what the skin’s own cycle is doing less efficiently. Regular treatment intervals help maintain the momentum of that renewal process rather than allowing surface pigmentation to build again between sessions.
How the Trexyne Peel Addresses Facial Dark Patches
The Trexyne Peel approaches facial pigmentation through a botanical, mechanical resurfacing mechanism. Its active component is marine algae spicules, which are microscopic structures that create controlled micro-channels across the skin surface when applied by a trained practitioner. This physical action stimulates the skin’s renewal response, accelerating cell turnover and supporting the progressive shedding of pigmented surface cells.
Because the mechanism is mechanical rather than chemical, the Trexyne Peel does not introduce the inflammatory signals associated with more aggressive resurfacing approaches. For clients where inflammation is already a driver of pigmentation, this distinction is clinically meaningful. The treatment supports renewal without adding the kind of tissue stress that can, in some cases, worsen hyperpigmentation rather than improve it.
Stabilised Vitamin E and Skin Recovery
The formulation also includes stabilised tocopherol, a form of Vitamin E that may support the skin’s recovery phase from the first application. This helps maintain skin integrity throughout the resurfacing process, which is particularly relevant for clients with reactive or pigmentation-prone skin who need their skin to recover well between sessions.
Tiered Protocol for Different Presentations
The Trexyne Peel uses a tiered protocol that allows practitioners to match treatment intensity to the client’s skin type, history, and tolerance. This is not a one-size approach. Clients with sensitive or highly reactive skin can be treated at a lower intensity to begin with, while those with more resilient skin and well-established surface pigmentation can be treated more assertively from the outset. This adaptability makes the Trexyne Peel a versatile tool across a range of pigmentation presentations.
Assessing a Client With Facial Dark Patches
A thorough consultation is the foundation of any effective pigmentation programme. Without understanding the likely cause, the depth of the pigmentation, and the client’s skin profile, it is difficult to make reliable treatment decisions.
Key questions to cover during assessment include the history and timeline of the patches, whether they are new, stable, or worsening, any hormonal changes or medications that may be relevant, the client’s sun protection habits, their history with skincare products and any previous treatments, and whether they have experienced inflammatory skin conditions such as acne or eczema.
The distribution and appearance of the patches also provide useful diagnostic clues. Symmetrical, diffuse patches across the mid-face point toward melasma. Well-defined, isolated spots in high-UV-exposure areas suggest solar lentigines. Irregular patches following resolved acne or breakouts indicate PIH.
Building a Treatment Programme for Dark Patches
Once the cause and presentation are understood, a structured programme can be built around that assessment. For most clients with facial dark patches, a course of resurfacing treatments rather than a single session produces the best visible improvement.
Practitioners can explore the full range of available pack sizes and pricing for the Trexyne Peel via the Trexyne shop. Options run from a single 30ml vial to courses of 10 and 20 peels, which suits both individual assessment sessions and longer-term pigmentation programmes for clients who need sustained treatment over several months.
Treatment intervals, home care recommendations, and SPF protocol should all be mapped out at the outset so clients understand what is required of them between appointments. The more invested clients are in the full programme, the more reliable the results tend to be.
For practitioners who would like to discuss clinical approaches or have specific questions about using the Trexyne Peel for facial hyperpigmentation, the team is available via the contact page.
Lifestyle Factors That Contribute to Facial Dark Patches
Beyond the primary clinical triggers, several lifestyle factors can compound pigmentation or slow the rate at which it responds to treatment.
Heat exposure is worth raising with clients, particularly those with suspected melasma. Saunas, steam rooms, prolonged hot baths, and even vigorous exercise that generates significant facial heat have been associated with worsening melasma in susceptible individuals. This does not mean clients need to avoid all heat, but they should be aware of it as a potential aggravating factor during an active treatment course.
Chronic stress has a systemic inflammatory effect that can influence skin behaviour, including pigmentation patterns in susceptible skin. It is not always within scope to address directly, but acknowledging it as a contributing factor helps clients take a more complete view of their skin health.
Skincare habits matter too. Picking, squeezing, or aggressively rubbing at areas of existing pigmentation can cause low-level trauma that triggers further melanin production. Clients should be guided toward a gentle, intentional routine that supports rather than disrupts the work being done in the treatment room.
More information about the Trexyne Peel’s approach to professional skin resurfacing is available at Trexyne.com.
Conclusion
Dark patches on the face develop when the skin’s melanocytes become overactive in response to a specific trigger. UV exposure drives the formation of solar lentigines through cumulative damage over time. Hormonal changes, particularly elevated oestrogen, are associated with melasma and its characteristic symmetrical patches. Post-inflammatory hyperpigmentation follows any localised inflammatory event, with acne being the most common cause in clinical practice. Certain medications, ageing, and slowing cell turnover all contribute to how visible these patches become and how persistent they are.
Effective management depends on identifying the cause, addressing the ongoing triggers, and supporting the skin’s renewal process with the right professional treatment. The Trexyne Peel offers a botanical, mechanically driven resurfacing option that may help progressively improve the appearance of facial dark patches. Its marine algae spicule mechanism stimulates cell renewal without chemical exfoliants, its stabilised Vitamin E may support the skin’s recovery between sessions, and its tiered protocol allows treatment to be calibrated to each individual presentation. Used as part of a wider strategy that includes consistent sun protection and appropriate home care, it may support clients in achieving a noticeably brighter, more even-looking complexion over time.
Frequently Asked Questions
Q: What are the most common causes of dark patches on the face?
The most common causes are cumulative UV exposure leading to solar lentigines, hormonal changes driving melasma, and post-inflammatory hyperpigmentation following acne or other skin trauma. Less commonly, certain medications are associated with pigmentation changes. In most cases, more than one factor is contributing, which is why a thorough consultation before starting any treatment programme is important.
Q: Can hormonal changes cause dark patches on the face to appear suddenly?
Yes. Hormonal shifts, particularly increases in oestrogen, can trigger melasma relatively quickly. Clients often notice the onset during pregnancy, after starting hormonal contraception, or in association with their menstrual cycle. The symmetrical, diffuse pattern of melasma across the cheeks, forehead, and upper lip is often the first visible sign of hormonally driven pigmentation.
Q: What is the difference between dark patches caused by sun damage and those caused by hormones?
Sun-related dark patches, or solar lentigines, tend to be well-defined, isolated spots that cluster in areas of high UV exposure such as the cheeks, nose, and forehead. They tend to develop gradually over years. Hormonal patches associated with melasma are typically more diffuse, symmetrical, and spread across the central face. They can develop more rapidly, particularly around significant hormonal events.
Q: Is the Trexyne Peel suitable for treating dark patches caused by post-inflammatory hyperpigmentation?
The Trexyne Peel may support the gradual improvement of post-inflammatory hyperpigmentation through its mechanical resurfacing mechanism, which stimulates cell renewal without introducing additional inflammatory stress. This makes it a considered option for clients where treatment-induced inflammation could otherwise risk worsening the pigmentation. A thorough consultation, patch test, and conservative starting protocol are recommended, particularly for clients with ongoing acne or highly reactive skin.
Q: How long does it take for professional resurfacing to improve dark patches on the face?
Results vary depending on the type of pigmentation, its depth, and how consistently the client adheres to the full programme including SPF use and home care. Surface-level post-inflammatory pigmentation may begin to show visible improvement after a small number of sessions. Solar lentigines and melasma typically require a more sustained course of treatment before meaningful change is apparent. Most practitioners recommend committing to a full course rather than assessing results after one or two sessions.
Q: Can dark patches on the face be completely removed, or just faded?
For many clients, significant visible fading is achievable with a well-structured treatment programme. Complete removal is less predictable, particularly for deeper pigmentation or conditions with ongoing hormonal or UV drivers. Setting realistic expectations is an important part of the consultation process. For most presentations, the goal is a progressively more even-looking skin tone maintained through ongoing management rather than a single permanent correction.
Q: Where can practitioners buy the Trexyne Peel for treating facial hyperpigmentation?
The Trexyne Peel is available exclusively to verified practitioners and clinics through the Trexyne shop. Pricing starts at £175.00 for a single 30ml vial, which provides approximately 6 to 8 full-face treatments. Course packs of 10 and 20 peels are also available for practitioners running structured pigmentation programmes. For clinical queries or purchasing enquiries, you can reach the team via the contact page.