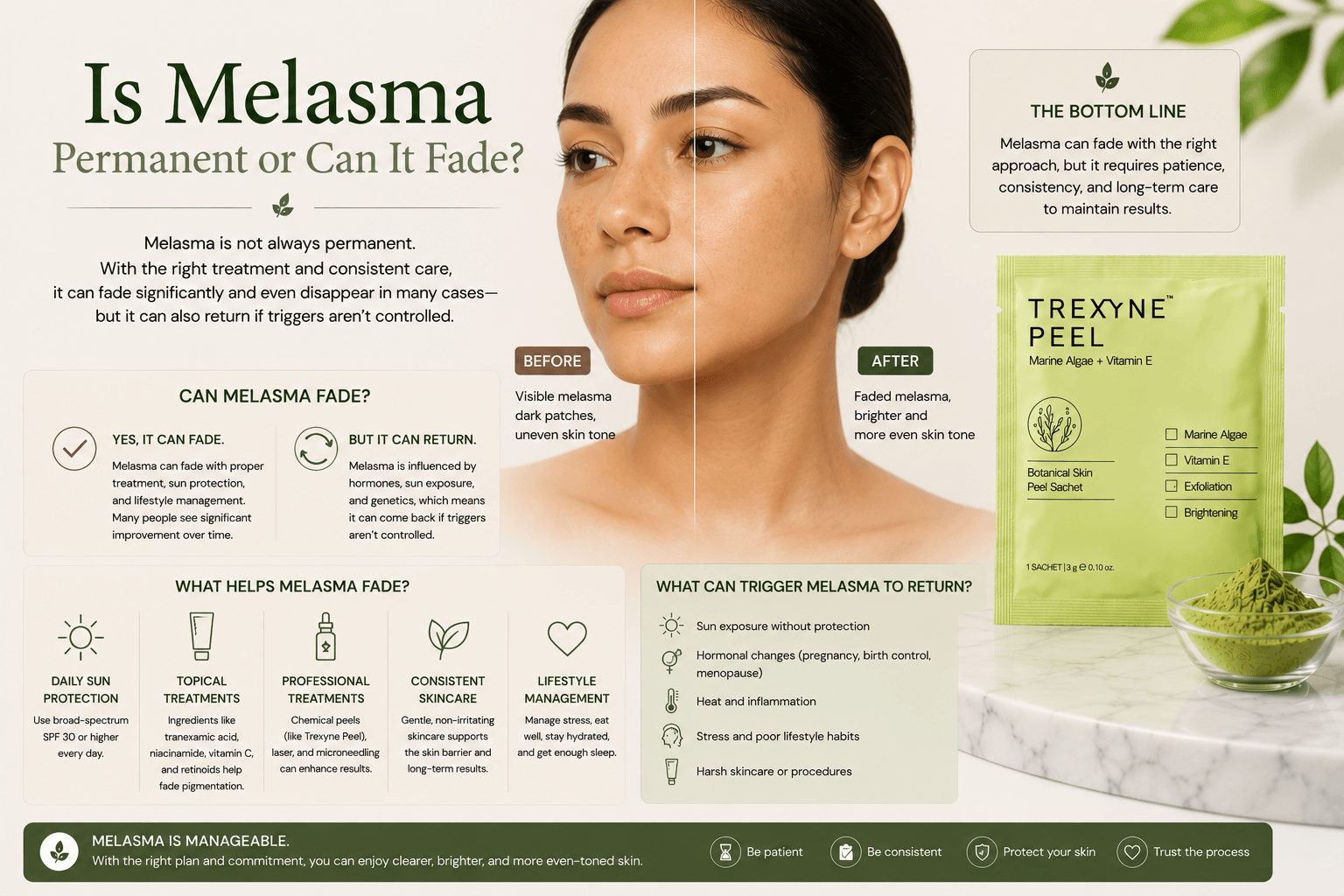
Is Melasma Permanent or Can It Fade?
Melasma is not necessarily permanent, but it is a chronic condition that is managed rather than cured. For some clients it fades significantly on its own when the hormonal trigger that drove it is removed, for example after pregnancy ends or after stopping hormonal contraception. For many others, particularly those with long-standing melasma or a persistent hormonal driver, it does not resolve without professional intervention and requires ongoing management to maintain visible improvement. The honest clinical answer is that complete, lasting clearance of melasma is uncommon, but meaningful visible improvement is achievable for most clients through the right combination of professional treatment, rigorous daily sun protection, and trigger management. For practitioners building a treatment plan, professional resurfacing options such as the Trexyne Peel can support this improvement, but they work most effectively when they form part of a broader management approach rather than being relied upon as a standalone fix.
Why Melasma Is Not Simply a Permanent Condition
The word permanent implies a fixed, irreversible state. Melasma is neither fixed nor irreversible for most clients. It is a dynamic condition that responds to changes in its triggers. When those triggers are reduced or removed, the condition often improves. When those triggers are sustained or increase, it worsens.
This dynamic quality is one of the most clinically important things to understand about melasma, because it shapes both treatment planning and the conversation with clients about realistic outcomes. A client who understands that their melasma is likely to improve significantly if the relevant triggers are managed will approach treatment differently from one who believes the condition is permanent and therefore untreatable.
The reason melasma is described as chronic rather than permanent is that even when improvement is achieved, the predisposition to the condition does not disappear. Clients with a history of melasma who achieve significant fading through professional treatment and rigorous sun protection remain susceptible to recurrence if hormonal triggers return or UV exposure increases substantially. Sustaining improvement requires ongoing management rather than a single treatment course followed by a return to previous habits.
When Melasma Fades on Its Own
The most common scenario in which melasma fades without professional intervention is after pregnancy. Pregnancy-related melasma, sometimes called chloasma or the mask of pregnancy, develops because elevated oestrogen and progesterone sensitise melanocytes to UV stimulus. After delivery, as hormone levels begin to normalise over the weeks and months that follow, melanocyte activity in the affected areas often decreases and the pigmentation partially or sometimes substantially fades.
The extent of fading varies significantly between individuals. Some clients find their pregnancy-related melasma has faded to near-invisibility within six months of delivery. Others find it persists at a level that still concerns them, particularly if the patches were deep or extensive before delivery. Epidermal melasma, where pigment sits in the upper layers of the skin, tends to fade more readily than mixed or dermal presentations where pigment has been deposited more deeply.
Similarly, clients who develop melasma in association with hormonal contraception sometimes find that it fades after stopping the contraceptive. However, this is not universal. Melasma that has been present for a longer period, or where UV exposure has been significant during the period of hormonal stimulation, tends to have a more established pigmentation pattern that does not resolve spontaneously when the hormonal trigger is removed.
When Professional Treatment Is Needed
For clients whose melasma does not resolve on its own after the hormonal trigger is removed, or for those who are managing melasma while the hormonal trigger remains active, professional treatment is typically needed to achieve visible improvement. The condition does not worsen indefinitely in all cases, but it rarely improves spontaneously to a degree that satisfies most clients without active intervention.
Professional resurfacing supports fading by stimulating cell turnover and progressively displacing the pigmented cells in affected areas with fresh, unpigmented ones. The rate of improvement depends on the depth of the pigmentation, the consistency of sun protection, whether the hormonal trigger is still active, and how well the skin tolerates and responds to the resurfacing approach used.
For melasma specifically, the choice of resurfacing mechanism matters considerably. Treatments that generate a significant chemical inflammatory response carry a risk of restimulating the melanocyte activity they are attempting to reduce. The Trexyne Peel resurfaces through marine-algae spicules using a purely mechanical mechanism, avoiding the chemical inflammatory trigger that can cause a rebound worsening of melasma in susceptible skin. Stabilised Vitamin E in the formulation supports recovery, further reducing the inflammatory load during the inter-session window when melasma-prone skin is particularly vulnerable to triggers.
The Difference Between Epidermal and Dermal Melasma
Whether melasma can fade, and how fully, is significantly influenced by where the pigment sits within the skin. This is one of the most practically important distinctions in melasma management, and it is worth explaining clearly to clients before any treatment course is planned.
Epidermal melasma involves pigment deposited in the upper layers of the epidermis, where cell turnover naturally brings it progressively closer to the surface over time. This type of melasma has the best prognosis for fading, both spontaneously and in response to professional resurfacing. It appears brown rather than grey in natural light, and it responds relatively clearly to UV light assessment techniques that allow practitioners to visualise pigmentation depth.
Dermal melasma involves pigment that has been deposited in the dermis, deeper than the epidermis. Resurfacing treatments work by stimulating epidermal renewal, which cannot directly address dermal pigmentation. Dermal melasma is far more resistant to topical and resurfacing treatments than epidermal melasma, and it tends to appear grey or blue-grey rather than brown. Complete resolution of dermal melasma is uncommon, though the condition may be partially manageable through other approaches.
Mixed melasma involves both epidermal and dermal components, producing a partial response to resurfacing where the epidermal portion improves while the dermal component does not. Clients with mixed presentations may see significant but incomplete improvement from a professional course, which can be frustrating if the expectation was full resolution. Managing this expectation honestly before treatment is a clinical and ethical responsibility.
The Role of Sun Protection in Whether Melasma Fades
The single most significant factor in whether melasma fades and stays faded is consistent daily sun protection. UV exposure is the primary environmental amplifier of melasma activity, and without adequate ongoing protection, even successfully treated melasma will return.
Clients who achieve meaningful improvement through professional treatment and then relax their SPF habits in the months that follow consistently experience recurrence, sometimes within a few weeks of significant UV exposure. This recurrence can be demoralising and may lead clients to conclude that treatment did not work, when the more accurate explanation is that the treatment worked but the results were not protected afterwards.
Daily broad-spectrum SPF with meaningful UVA coverage applied every morning without exception is the foundation of any melasma management plan. It is not supplementary to professional treatment. It is a clinical requirement for professional treatment to produce and sustain visible results.
What Realistic Improvement Looks Like
For clients with epidermal melasma who are committed to daily sun protection, trigger management, and a sustained professional treatment course, meaningful visible improvement is a realistic outcome. This typically means a noticeable lightening of the affected patches, a reduction in the contrast between the melasma areas and the surrounding skin, and an overall more even-looking complexion across the treated areas.
The word meaningful is important here because the degree of improvement varies. Some clients achieve results that leave their melasma barely visible in everyday lighting. Others achieve significant fading that is clearly visible in photographs but that does not fully resolve to a completely even tone. For clients with long-standing or deep melasma, partial improvement that represents a substantial change from their starting point is a clinically realistic and valuable outcome even if it falls short of complete resolution.
The timeline for visible improvement is slow compared to other pigmentation concerns. Progress builds across multiple sessions and may be most clearly apparent when comparing photographs taken at the start of the course with those taken several months into it, rather than assessing day-to-day changes.
Managing Client Expectations Honestly
The conversation about whether melasma is permanent is one that practitioners need to handle carefully. Being overly optimistic risks setting up unrealistic expectations that undermine the client relationship when results are less complete than hoped. Being overly pessimistic may discourage clients from pursuing treatment that could genuinely improve their quality of life and confidence.
The balanced, accurate message is that melasma is a manageable condition for most clients, that meaningful visible improvement is achievable with the right approach and consistent trigger management, and that the condition is likely to require ongoing management rather than a single course of treatment to resolve once and for all.
Practitioners who deliver this message clearly and compassionately, and who then execute a well-planned treatment course with appropriate intensity and session spacing, give their clients the best possible chance of a positive experience and outcome.
Practitioners interested in incorporating the Trexyne Peel into their melasma management protocols can explore the full product range via the Trexyne shop, or get in touch with the Trexyne team directly through the Trexyne contact page.
When to Seek Dermatological Input
For clients whose melasma is extensive, deeply established, or has failed to respond to multiple well-managed professional treatment courses, dermatological referral is appropriate before further aesthetic treatment is planned. A dermatologist can assess pigmentation depth using specialist tools, consider prescription topical treatments or systemic management of hormonal triggers, and advise on whether the likely presentation is epidermal, dermal, or mixed.
Referral is also appropriate for clients who are managing melasma alongside other skin conditions, or who are using prescription medications that may be contributing to the hormonal driver. The aesthetic practitioner’s role in these cases is to recognise the limits of their remit and to facilitate appropriate medical input rather than to manage everything within the clinic setting.
More information on the Trexyne approach to professional botanical resurfacing is available on the Trexyne website.
Conclusion
Melasma is not permanently fixed for most clients, but it is a chronic condition that requires ongoing management rather than a single treatment to resolve. It can fade on its own when the hormonal trigger is removed, particularly after pregnancy, but many clients require professional intervention to achieve meaningful visible improvement, especially where the condition is long-standing or where a persistent hormonal driver remains active. Epidermal melasma responds better to resurfacing than dermal presentations, and the choice of resurfacing mechanism matters significantly for a condition that can be worsened by chemical inflammatory triggers. The Trexyne Peel offers a mechanical approach that supports progressive cell turnover without that inflammatory risk, with stabilised Vitamin E supporting recovery during the inter-session window. With realistic expectations, rigorous daily sun protection, and a well-managed professional treatment course, meaningful visible improvement and a brighter, more even-looking complexion are achievable outcomes for most clients with epidermal melasma.
FAQs
Q: Is melasma permanent or can it fade?
Melasma is not necessarily permanent. It can fade on its own when the hormonal trigger is removed, such as after pregnancy, and it can improve significantly with professional treatment and rigorous sun protection. However, it is a chronic condition, and the predisposition to it does not disappear even when improvement is achieved. Ongoing management is needed to sustain results.
Q: Can melasma go away without treatment?
For some clients, particularly those whose melasma developed during pregnancy or in association with hormonal contraception, the condition fades significantly after the hormonal trigger is removed. However, this is not universal, and long-standing or deep melasma often persists without professional intervention. Even where some spontaneous fading occurs, professional treatment and consistent sun protection typically produce better outcomes than waiting alone.
Q: Why does melasma come back after it has faded?
Melasma returns when the triggers that originally produced it, primarily UV exposure and hormonal activity, continue to act on skin that remains predisposed to the condition. Clients who relax their sun protection habits after successful treatment often experience recurrence within weeks of significant UV exposure. Ongoing daily SPF use and periodic maintenance sessions are needed to sustain improvement over the long term.
Q: What type of melasma is easiest to treat?
Epidermal melasma, where pigment sits in the upper layers of the skin, responds best to professional resurfacing and has the most favourable prognosis for visible fading. Dermal melasma, where pigment has deposited in the deeper dermis, is largely beyond the reach of resurfacing and is much more resistant to improvement. Mixed presentations respond partially, with the epidermal component improving while the dermal component does not.
Q: How long does it take for melasma to fade with professional treatment?
Progress from professional resurfacing for melasma is gradual, building across multiple sessions over several months rather than appearing quickly after a few appointments. Visible improvement is often most apparent when comparing photographs from the start of the course with those taken several months later. The timeline depends on the depth of the pigmentation, how consistently sun protection is maintained, and whether a hormonal trigger remains active during treatment.
Q: Can the Trexyne Peel help melasma fade?
The Trexyne Peel can support gradual improvement in epidermal melasma by stimulating cell turnover through a mechanical mechanism that avoids the chemical inflammatory trigger most likely to worsen the condition. Results build progressively across a sustained course, and consistent daily broad-spectrum SPF use throughout is essential to protect the improvement being achieved between sessions.
Q: Does melasma eventually stop getting worse on its own?
In some clients, melasma reaches a plateau rather than worsening indefinitely, particularly when UV exposure and hormonal factors are well managed. However, this plateau can still represent a significant level of visible pigmentation that most clients want to address professionally. Without active management, melasma rarely resolves on its own in clients with established or persistent presentations.