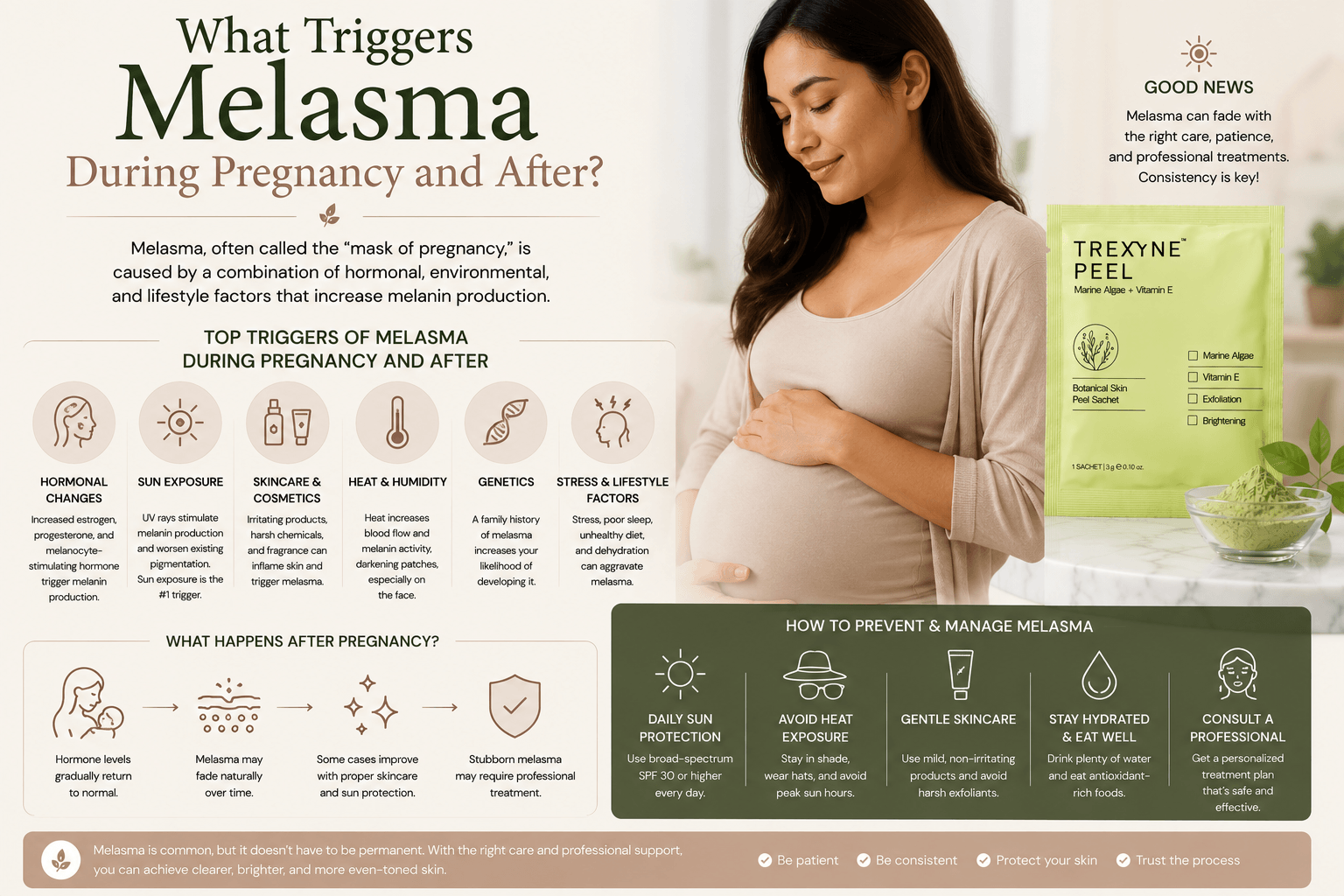
What Triggers Melasma During Pregnancy and After?
Melasma during pregnancy is driven by a specific hormonal sequence that significantly amplifies how the skin’s melanocytes respond to UV exposure. The condition is common enough during pregnancy to have earned its own name, chloasma, and affects a substantial proportion of pregnant women to some degree. Understanding exactly what triggers it during pregnancy, why it behaves differently after delivery for different women, and when professional resurfacing becomes appropriate in the post-natal period, are all clinically relevant questions for practitioners working with this client group. The Trexyne Peel can form part of a post-natal management plan for persistent melasma, but only at the right point in the hormonal and recovery timeline. This post explains what that timeline looks like and what drives each stage of it.
The Hormonal Sequence That Triggers Melasma During Pregnancy
Pregnancy involves a dramatic and sustained rise in several hormones, most significantly oestrogen, progesterone, and melanocyte-stimulating hormone. Each of these plays a role in the development of melasma during pregnancy, and their combined effect is considerably greater than any single hormone would produce alone.
Oestrogen stimulates melanocyte activity directly and also increases the skin’s sensitivity to other pigmentation triggers. Progesterone has a similar sensitising effect on melanocytes, increasing their responsiveness to UV radiation and to the inflammatory signals that can also provoke melanin production. Melanocyte-stimulating hormone, which rises particularly in the second and third trimesters, directly prompts melanocytes to produce melanin as part of a broader hormonal pattern that also causes the darkening of the areolae, linea nigra, and other pigmented areas of the body that are characteristic of pregnancy.
The result of this combined hormonal environment is a set of melanocytes that are far more reactive than they would normally be. When UV radiation, the primary environmental trigger for melanin production, reaches skin that is in this primed hormonal state, the melanocyte response is disproportionately large. Patches of concentrated melanin develop across the areas with the highest density of sun-sensitive melanocytes, typically the central face, producing the characteristic symmetrical distribution of chloasma.
Why Some Women Develop Melasma During Pregnancy and Others Do Not
Not every pregnant woman develops melasma, and the variation between individuals reflects several factors that interact with the shared hormonal environment of pregnancy.
Skin type is the most consistently relevant factor. Fitzpatrick types III to VI, which encompass medium, olive, brown, and darker skin tones, have higher baseline melanocyte density and reactivity. In the hormonal environment of pregnancy, these skin types are significantly more likely to develop visible melasma than Fitzpatrick types I and II. The underlying predisposition is biological rather than behavioural, though UV habits significantly influence how severe the outcome is.
UV exposure habits during pregnancy are the most significant modifiable risk factor. Women who spend significant time outdoors without adequate sun protection, or who live in high UV environments, are considerably more likely to develop pronounced melasma than those with consistent, rigorous protection. The hormonal priming is the same regardless of UV habits, but UV exposure is the trigger that converts that priming into visible pigmentation. Without sufficient UV stimulus, even hormonally primed melanocytes may not produce enough excess melanin to create visible patches.
Genetic predisposition also plays a role. Women with a family history of melasma, or who have experienced it in a previous pregnancy, are more likely to develop it again. The underlying tendency for melanocytes to respond strongly to hormonal and UV triggers is partly inherited.
Previous use of hormonal contraception that produced melasma is another risk indicator. If the hormonal changes of oral contraception were sufficient to trigger visible melasma, the far more pronounced hormonal shifts of pregnancy are likely to do so as well.
What Happens to Melasma After Delivery
The hormonal environment of pregnancy begins to change rapidly after delivery. Oestrogen and progesterone levels drop significantly in the days and weeks following birth, and melanocyte-stimulating hormone also decreases as the post-partum hormonal rebalancing takes place. For many women, this hormonal shift is accompanied by some degree of spontaneous fading of the melasma that developed during pregnancy.
The extent and speed of this fading varies considerably. Some women find their melasma has largely resolved within three to six months of delivery. Others find it persists with only minor change, particularly if the pigmentation was deep or extensive during pregnancy, or if post-natal UV exposure has been unprotected. Women who continue breastfeeding may find that hormonal levels normalise more slowly during the breastfeeding period, which can mean melasma fades more gradually than in women who do not breastfeed.
The depth of the pigmentation at the time of delivery influences how readily it fades. Epidermal melasma, where melanin is concentrated in the upper layers of the skin, fades more readily as normal cell turnover brings pigmented cells progressively towards the surface. Deeper or mixed presentations, where melanin has been deposited across both epidermal and dermal layers, are less likely to resolve fully through spontaneous fading alone.
Why Post-Natal Hormonal Changes Affect Treatment Timing
Understanding the post-natal hormonal timeline is essential for practitioners advising clients on when to begin professional resurfacing for persistent melasma. Starting a resurfacing course too early, before hormonal levels have had time to stabilise, means the active hormonal trigger may still be partially or fully active during treatment. This limits how much visible progress the treatment can make and increases the risk of new pigmentation developing between sessions even as existing patches are being addressed.
As a general principle, allowing at least three to six months after delivery for hormonal levels to begin normalising before starting professional resurfacing is a more reliable approach than beginning immediately post-natal. For women who are breastfeeding, deferring further until after breastfeeding has ended is appropriate, since breastfeeding maintains elevated prolactin and somewhat altered oestrogen levels that may sustain melanocyte sensitivity.
This deferral period is not simply waiting for the sake of it. It is the point at which the practitioner can make a more accurate assessment of the actual residual melasma once the acute hormonal stimulus has reduced, and where any spontaneous fading that is going to occur has had time to do so. Starting treatment at this point means working with a more stable picture of the concern and a more settled hormonal environment.
The Role of UV Exposure in Post-Natal Melasma
Post-natal UV exposure is often underestimated as a factor in whether melasma persists or worsens after pregnancy. Many women are focused on the demands of early parenthood and may not prioritise the sun protection habits that are essential for protecting recovering skin from further pigmentation stimulus.
Even after delivery, melanocytes in previously affected areas retain a degree of the sensitisation they developed during pregnancy. UV exposure continues to be a significant trigger for melanin production in these areas, particularly in the months immediately after delivery when hormonal levels are still fluctuating. Without consistent daily SPF use, the melasma that was present during pregnancy can deepen or extend rather than fading as hormone levels normalise.
Daily broad-spectrum SPF should be recommended to post-natal clients with melasma from the earliest possible point after delivery, regardless of whether professional resurfacing is being considered or deferred. This is the single most impactful step available during the post-natal waiting period, and it protects whatever spontaneous fading may occur from being reversed by ongoing UV stimulus.
When to Begin Professional Resurfacing Post-Natally
Once the appropriate post-natal waiting period has been observed and the skin has been assessed, professional resurfacing for persistent melasma can be considered. The assessment at this point should establish how much residual melasma is present after spontaneous post-natal fading, what the depth and distribution of the remaining pigmentation appears to be, and whether the client’s barrier and overall skin condition are in a suitable state to receive resurfacing.
The Trexyne Peel is a relevant option for post-natal melasma management because its mechanical resurfacing mechanism avoids the chemical inflammatory trigger that is most likely to worsen melasma in hormonally sensitised skin. Even after delivery and hormonal stabilisation, post-natal skin that has carried melasma through a pregnancy retains a degree of melanocyte reactivity that makes it more vulnerable to inflammatory restimulation than skin without this history.
The stabilised Vitamin E in the formulation supports recovery, and the tiered protocol allows practitioners to begin conservatively and progress only as the skin demonstrates its tolerance. This graduated approach is particularly appropriate for post-natal skin, which may be more variable in its condition from session to session than skin that has not been through the physiological demands of pregnancy and early parenthood.
Managing Realistic Expectations With Post-Natal Clients
Post-natal clients managing persistent melasma are often dealing with significant life demands alongside a skin concern that is affecting their confidence. Balancing honest clinical expectation-setting with genuine empathy for their situation requires a thoughtful approach.
The key messages to communicate are that professional resurfacing at the right time in the post-natal timeline can produce meaningful visible improvement, that results will build gradually rather than appearing quickly, and that daily SPF use is as important as the professional treatment in determining how well results are sustained. Clients who understand why the timing matters and why they are being asked to wait before starting a course are more likely to feel clinically supported rather than dismissed.
For clients who experienced significant melasma during pregnancy and are concerned about it recurring in a future pregnancy, honest communication about the likelihood of recurrence is also appropriate. Melasma that developed during one pregnancy is likely to return in subsequent pregnancies, and pre-pregnancy sun protection habits and prompt post-natal management are the practical tools available to limit its impact.
Practitioners looking to incorporate the Trexyne Peel into their post-natal melasma protocols can explore the full product range through the Trexyne shop, or contact the team directly via the Trexyne contact page.
When Post-Natal Melasma Requires Dermatological Input
Most post-natal melasma is appropriate for management within the aesthetic clinic setting once the hormonal timeline has been respected and the skin has been properly assessed. However, some presentations warrant dermatological input before professional resurfacing is considered.
Extensive or very deep melasma that has been present throughout the pregnancy and shows little spontaneous fading post-natally may involve a significant dermal component that resurfacing alone cannot address. Clients with a history of treatment-resistant melasma from before their pregnancy benefit from dermatological assessment of pigmentation depth before committing to a further resurfacing course.
Clients with post-natal skin conditions unrelated to melasma, such as a significant eczema flare or an inflammatory skin reaction that has developed during or after pregnancy, should have these assessed and managed before any resurfacing is considered in the affected areas.
More information on the Trexyne approach to professional botanical resurfacing is available on the Trexyne website.
Conclusion
Melasma during pregnancy is triggered by the combined effect of elevated oestrogen, progesterone, and melanocyte-stimulating hormone, which prime melanocytes to respond disproportionately to UV exposure and produce the characteristic symmetrical pigmentation of chloasma. After delivery, hormonal levels begin to normalise and some spontaneous fading often occurs, but the extent and speed of this fading varies significantly between individuals. Post-natal professional resurfacing should be deferred until hormonal levels have had time to stabilise and, where applicable, until breastfeeding has ended. At that point, the Trexyne Peel can form part of a carefully managed treatment plan for persistent melasma, using a mechanical mechanism that avoids inflammatory restimulation of already-sensitised melanocytes, with stabilised Vitamin E supporting recovery and a tiered protocol allowing conservative progression. With consistent daily SPF, appropriate timing, and realistic expectations, it may support meaningful improvement in post-natal melasma and contribute to a brighter, more even-looking complexion as part of a thoughtful long-term management plan.
FAQs
Q: What triggers melasma during pregnancy?
Melasma during pregnancy is triggered by a combination of elevated oestrogen, progesterone, and melanocyte-stimulating hormone, which sensitise melanocytes to produce disproportionately large amounts of melanin in response to UV exposure. The areas most affected are typically those with the highest density of sun-sensitive melanocytes, producing the characteristic symmetrical patches across the cheeks, forehead, and upper lip.
Q: Why do some pregnant women get melasma and others do not?
Skin type, UV exposure habits, genetic predisposition, and previous hormonal history all influence whether a pregnant woman develops visible melasma. Fitzpatrick types III to VI are significantly more susceptible, and women with a family history of melasma or who have experienced it with hormonal contraception are at higher risk. Consistent UV protection during pregnancy substantially reduces the risk of visible melasma developing even in susceptible skin types.
Q: Does melasma go away after pregnancy?
For many women, melasma fades to some degree in the months after delivery as hormonal levels normalise. The extent of fading varies: some experience near-complete resolution within six months, while others retain persistent pigmentation that requires professional management. Epidermal melasma fades more readily than deeper presentations, and consistent post-natal SPF use significantly influences how much fading occurs.
Q: When is it safe to start a professional peel for melasma after pregnancy?
Allowing at least three to six months post-delivery for hormonal levels to stabilise is generally advisable before beginning professional resurfacing. For women who are breastfeeding, deferring until after breastfeeding ends is appropriate. Starting too early risks treating skin where the active hormonal trigger is still partially present, limiting progress and increasing the risk of new pigmentation between sessions.
Q: Can the Trexyne Peel be used for post-natal melasma?
The Trexyne Peel can form part of a post-natal melasma management protocol once the appropriate timing has been observed and the skin has been properly assessed. Its mechanical mechanism avoids the chemical inflammatory trigger most likely to worsen melasma in hormonally sensitised skin, and its tiered protocol allows conservative, gradual progression suited to post-natal skin that may be more variable in its condition than skin without a recent pregnancy history.
Q: Will melasma come back in a future pregnancy?
Melasma that developed during one pregnancy is likely to return in subsequent pregnancies, as the same hormonal sequence that triggered it the first time will recur. Rigorous daily sun protection throughout subsequent pregnancies substantially reduces the severity of recurrence, though it cannot prevent the hormonal priming that makes the skin more reactive. Post-natal management after each pregnancy can address the resulting pigmentation.
Q: Does breastfeeding affect when melasma fades after delivery?
Breastfeeding maintains elevated prolactin levels and somewhat altered hormonal balance compared to the post-natal baseline for women who are not breastfeeding. This can mean that melasma fades more gradually during the breastfeeding period, and that the full post-natal hormonal stabilisation occurs later than it would otherwise. This is one reason why deferring professional resurfacing until after breastfeeding is generally the more appropriate clinical approach.