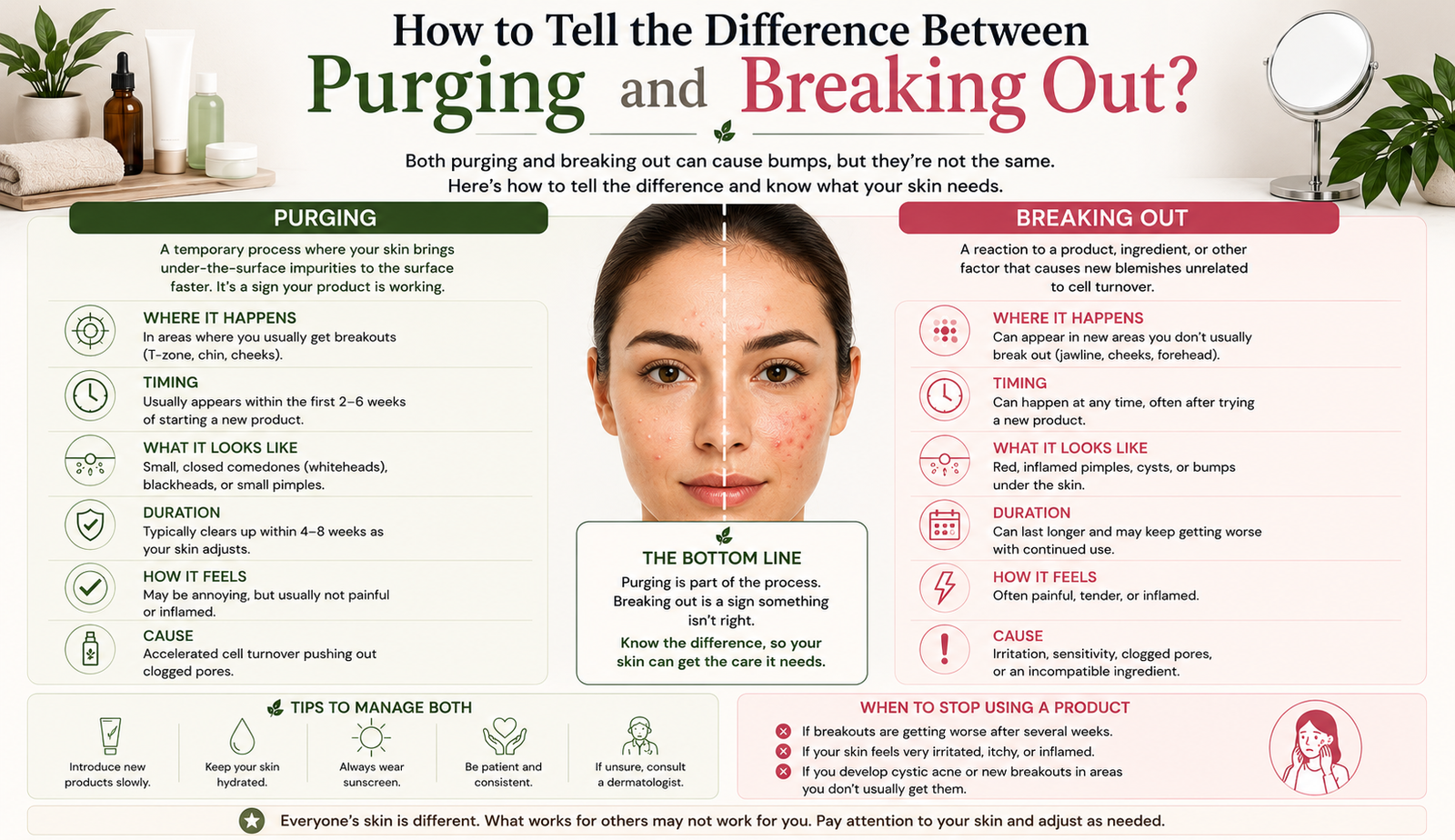
How to Tell the Difference Between Purging and Breaking Out?
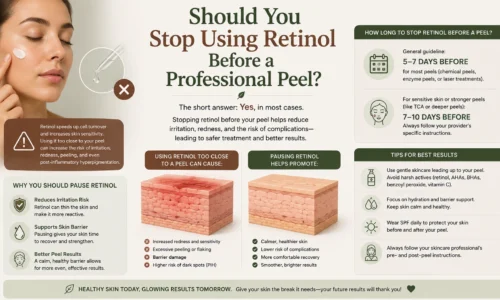
Purging and breaking out look similar on the surface but have different causes and different clinical implications. Understanding which one is happening matters because the appropriate response to each is different: purging typically resolves on its own as the skin adjusts to accelerated cell turnover, while a true breakout signals that something in the routine or treatment is not agreeing with the skin. Confusing the two leads clients to abandon effective treatment courses too early, or to persist with something that is genuinely irritating their skin when they should be stopping. The confusion is particularly common after professional resurfacing treatments, including mechanical options such as the Trexyne Peel, where accelerated cell turnover in the weeks following treatment can temporarily increase the visibility of congestion that was already present beneath the skin surface. This post explains what each is, how to distinguish them clinically, and what to do in each case.
What Skin Purging Actually Is
Purging refers to a temporary increase in breakout-like activity that occurs when cell turnover is significantly accelerated. When the skin renews itself faster than usual, congestion and comedones that were already developing beneath the surface are brought forward in the renewal cycle and become visible more quickly than they would have done at the skin’s normal rate of turnover. The result is a temporary cluster of breakouts that appear in the weeks following a treatment that has meaningfully increased cell turnover.
The critical distinction in purging is that the congestion was already there. The treatment has not created new blocked pores or triggered a new inflammatory response. It has accelerated the timeline by which existing subclinical comedones are surfacing. Once those pre-existing congested pores have cleared, the skin typically settles and looks clearer than it did before treatment, because the accelerated turnover has brought congestion to the surface and resolved it more quickly than the normal cycle would have allowed.
Purging is more commonly associated with topical actives such as retinoids, which specifically increase cell turnover as their primary mechanism. However, any resurfacing treatment that significantly accelerates cell turnover can produce a similar temporary surfacing effect in skin that is already congested beneath the surface. This is particularly relevant in the weeks following a professional resurfacing session.
What a True Breakout Is
A breakout, by contrast, involves the formation of new blocked pores and inflammatory lesions that were not already developing in the skin before the treatment or product was introduced. Something about the treatment, product, or circumstances has triggered a new inflammatory or comedogenic response rather than simply surfacing existing congestion more quickly.
Common triggers for a true breakout include products with comedogenic ingredients that block pores in susceptible skin, products or treatments that irritate the skin and provoke an inflammatory response, introducing too many new products at once so the specific cause is difficult to identify, and applying treatments to skin that is already inflamed or not in a suitable state to receive them.
A true breakout does not resolve cleanly in the same way purging does. Rather than clearing within a defined period as the pre-existing congestion is resolved, it can persist or worsen as new comedones and inflammatory lesions continue to form. It may also spread beyond the areas where congestion would typically surface, or produce lesion types that are different from the client’s usual breakout pattern.
The Key Distinguishing Features
Several observable features help distinguish purging from a true breakout, and a practitioner who can communicate these clearly to clients significantly reduces the risk of early treatment abandonment during what is actually a normal, transient surfacing response.
Location is one of the most reliable indicators. Purging typically occurs in areas where the individual already experiences congestion and breakouts. The accelerated turnover surfaces what was already there, so it appears in familiar zones. A true breakout may develop in areas where the client does not normally break out, which is a stronger indicator that something new is triggering comedone formation.
Lesion type also provides a clue. Purging typically produces the same types of blemishes the individual already experiences, predominantly blackheads, whiteheads, and small papules that reflect the type of congestion already present beneath the surface. If the reaction produces lesion types that are unusual for that individual, such as deep cysts in someone who normally only gets surface-level congestion, a true breakout is more likely.
Timeline is perhaps the most definitive differentiator. Purging is self-limiting. As the pre-existing congestion clears, the skin settles and improves. This typically occurs within four to six weeks of the initial increase in breakout activity, after which the skin is generally clearer. If breakout activity continues beyond this window without improvement, or worsens over time rather than settling, a true breakout is the more likely explanation.
How Professional Resurfacing Relates to Purging
Professional resurfacing treatments, including mechanical options such as the Trexyne Peel, accelerate cell turnover in the skin. In clients who have underlying congestion beneath the surface, this accelerated turnover can temporarily surface that congestion more visibly in the weeks following treatment.
This is not the Trexyne Peel causing a breakout. It is the accelerated renewal cycle bringing forward congestion that was already developing, in the same way that starting a retinoid can produce temporary purging in congested skin. The distinction matters enormously for client communication, because clients who see increased blemish activity in the weeks following their first resurfacing session often conclude the treatment is not agreeing with their skin and consider stopping.
The Trexyne Peel‘s mechanical mechanism does not introduce a comedogenic ingredient or a chemical irritant that would be expected to trigger new inflammatory breakout activity. If a client who has no history of congestion in a particular area develops new inflammatory lesions there following treatment, this warrants assessment as a potential reaction rather than purging. However, for clients with existing congestion who notice familiar blemish types surfacing in familiar zones within weeks of treatment, this is most consistent with purging rather than a breakout and should generally be allowed to resolve before any conclusions about the treatment are drawn.
Why This Distinction Is Critical for Client Retention
The purging versus breakout distinction is one of the most practically important pieces of information a practitioner can give a client at the start of a resurfacing course. Clients who are not forewarned about the possibility of temporary purging and then experience it are almost universally convinced that the treatment is causing their skin to break out. Many will stop the course before the purging has resolved, abandoning a treatment that was actually beginning to work.
Practitioners who explain the purging concept clearly at the initial consultation, and who set specific expectations about the likely timeline and what it should look like, dramatically reduce the risk of this premature abandonment. Telling a client that they may notice some familiar congestion surfacing in the weeks following their first session, that this is temporary and self-limiting, and that it is a different thing from the skin reacting badly to the treatment gives them the context to interpret what they are observing rather than drawing the worst conclusion from it.
This proactive communication also supports the practitioner-client relationship. Clients who feel their practitioner anticipated and explained their experience trust the practitioner’s clinical judgement more fully, which makes them more likely to follow subsequent guidance and to complete the treatment course.
When to Be Genuinely Concerned
While purging is a normal and self-limiting response, there are situations that warrant more careful assessment rather than reassurance that the skin is simply adjusting.
Blemishes appearing in areas where the client has no history of congestion, particularly if they are inflammatory rather than comedonal, are more consistent with a true reaction than with purging. Severe inflammation, deep cysts, or a distribution of lesions that does not match the client’s typical breakout pattern should be assessed clinically rather than attributed to purging without further investigation.
Blemish activity that worsens progressively beyond six to eight weeks of a new treatment course, rather than peaking and then settling, is more indicative of an ongoing trigger than a temporary surfacing response.
Any signs consistent with infection, including lesions that are unusually painful, warm, or accompanied by spreading redness or systemic symptoms, require medical assessment rather than aesthetic management.
In these situations, deferring further resurfacing sessions, reviewing the client’s full routine for potential comedogenic or irritating ingredients, and assessing whether the original treatment selection was appropriate for that individual’s skin are all part of a responsible clinical response.
Managing Home Care During a Purging Phase
For clients who are experiencing what is most likely purging following a professional resurfacing session, home care guidance during this period can support the resolution and reduce the risk of the congestion triggering a secondary inflammatory response.
Keeping the home routine stripped back and consistent is the most important advice. Adding new products during a purging phase increases the number of variables and makes it harder to determine whether the skin is responding normally or whether something in the routine is contributing to the activity. A gentle cleanser, a simple moisturiser, and daily SPF are the appropriate core routine during this period.
Avoiding the temptation to spot-treat aggressively or to introduce additional exfoliating products at home reduces the risk of over-treating skin that is already in an active renewal phase. This is a common instinctive response from clients who are uncomfortable with the increased blemish visibility, and it is counterproductive.
Maintaining SPF use is particularly relevant during and after a resurfacing course. Any inflammation associated with purging has the potential to produce post-inflammatory hyperpigmentation in susceptible skin types if UV exposure is not consistently protected against. This is especially relevant for clients with Fitzpatrick types III to VI who are undergoing resurfacing for pigmentation concerns.
Practitioners looking to incorporate clear pre and post-treatment communication into their Trexyne Peel protocols can explore the full product range via the Trexyne shop, or contact the team through the Trexyne contact page.
What to Do if You Are Not Sure Which Is Happening
Clients who are uncertain whether what they are experiencing is purging or a true breakout should contact their practitioner rather than making independent decisions about whether to continue or stop treatment. A practitioner who can assess the skin, the pattern of blemish activity, and the timeline relative to the treatment received is in a far better position to make this judgement than a client trying to interpret their own skin.
If in doubt, deferring the next resurfacing session while the practitioner assesses the situation is a reasonable precaution. Allowing an extra week or two for the skin to settle while a clearer picture of what is happening is established does not significantly set back a treatment course and is far preferable to either abandoning a course that was working or continuing to resurface skin that is having a genuine adverse reaction.
More information on the Trexyne approach to professional botanical resurfacing is available on the Trexyne website.
Conclusion
Purging and breaking out are frequently confused but clinically distinct responses. Purging is a temporary, self-limiting surfacing of pre-existing congestion driven by accelerated cell turnover, appearing in familiar zones, producing familiar blemish types, and resolving within four to six weeks as the pre-existing congestion clears. A true breakout involves new inflammatory or comedogenic activity triggered by an irritating or comedogenic product or treatment, tends to spread beyond familiar zones, and does not resolve cleanly within a defined window. Professional resurfacing treatments including the Trexyne Peel can produce temporary purging in clients with underlying congestion, and practitioners who explain this clearly at consultation significantly reduce the risk of clients abandoning effective treatment courses prematurely. With appropriate home care during the purging window and daily SPF to protect against post-inflammatory pigmentation, most clients move through this phase to clearer, more even-looking skin on the other side.
FAQs
Q: How do I tell if my skin is purging or breaking out?
The key differences are location, lesion type, and timeline. Purging occurs in areas where you already experience congestion, produces the same blemish types you normally get, and resolves within four to six weeks as pre-existing congestion clears. A true breakout can appear in new areas, may produce unusual lesion types for your skin, and does not settle cleanly within a defined window.
Q: Can a professional skin peel cause purging?
Professional resurfacing treatments that significantly accelerate cell turnover can temporarily surface pre-existing congestion that was already developing beneath the skin. This is a purging response rather than the treatment causing new breakouts. Clients with underlying congestion are more likely to notice this in the weeks following their first session, and it typically resolves as the pre-existing congestion clears.
Q: How long does purging last after a skin peel?
Purging following a professional resurfacing treatment typically peaks within the first two to four weeks after a session and resolves within four to six weeks as the pre-existing congestion is cleared by the accelerated renewal cycle. If blemish activity continues beyond this window or worsens rather than settling, a true reaction rather than purging is more likely and warrants assessment by the treating practitioner.
Q: Should I stop my skin treatment if I think I am purging?
Not immediately. If the blemish activity matches the characteristics of purging, appearing in familiar zones with familiar lesion types and following the expected timeline, continuing the treatment and allowing the purging phase to resolve is generally the appropriate approach. Contact your practitioner if you are unsure, or if the activity is severe, in unusual locations, or not improving within the expected timeframe.
Q: Can the Trexyne Peel cause breakouts?
The Trexyne Peel is a mechanical resurfacing treatment that does not use comedogenic ingredients or chemical irritants that would be expected to trigger new inflammatory breakout activity. Clients with underlying congestion may notice temporary purging as accelerated cell turnover surfaces pre-existing blemishes. Lesions appearing in areas without a history of congestion, or that are more inflammatory than the client’s typical pattern, warrant clinical assessment.
Q: How do I look after my skin during a purging phase?
Keep the routine stripped back to a gentle cleanser, a simple moisturiser, and daily SPF. Avoid introducing new products, adding exfoliating treatments at home, or aggressive spot treatment during this period. Maintaining daily sun protection is particularly important to prevent any inflammation from producing post-inflammatory pigmentation in susceptible skin types.
Q: What should I do if I cannot tell whether I am purging or breaking out?
Contact your practitioner. A clinical assessment of the blemish pattern, location, and timeline relative to the treatment received is far more reliable than self-assessment. If in doubt, deferring the next session while the skin is assessed is a reasonable precaution that does not significantly set back a treatment course.