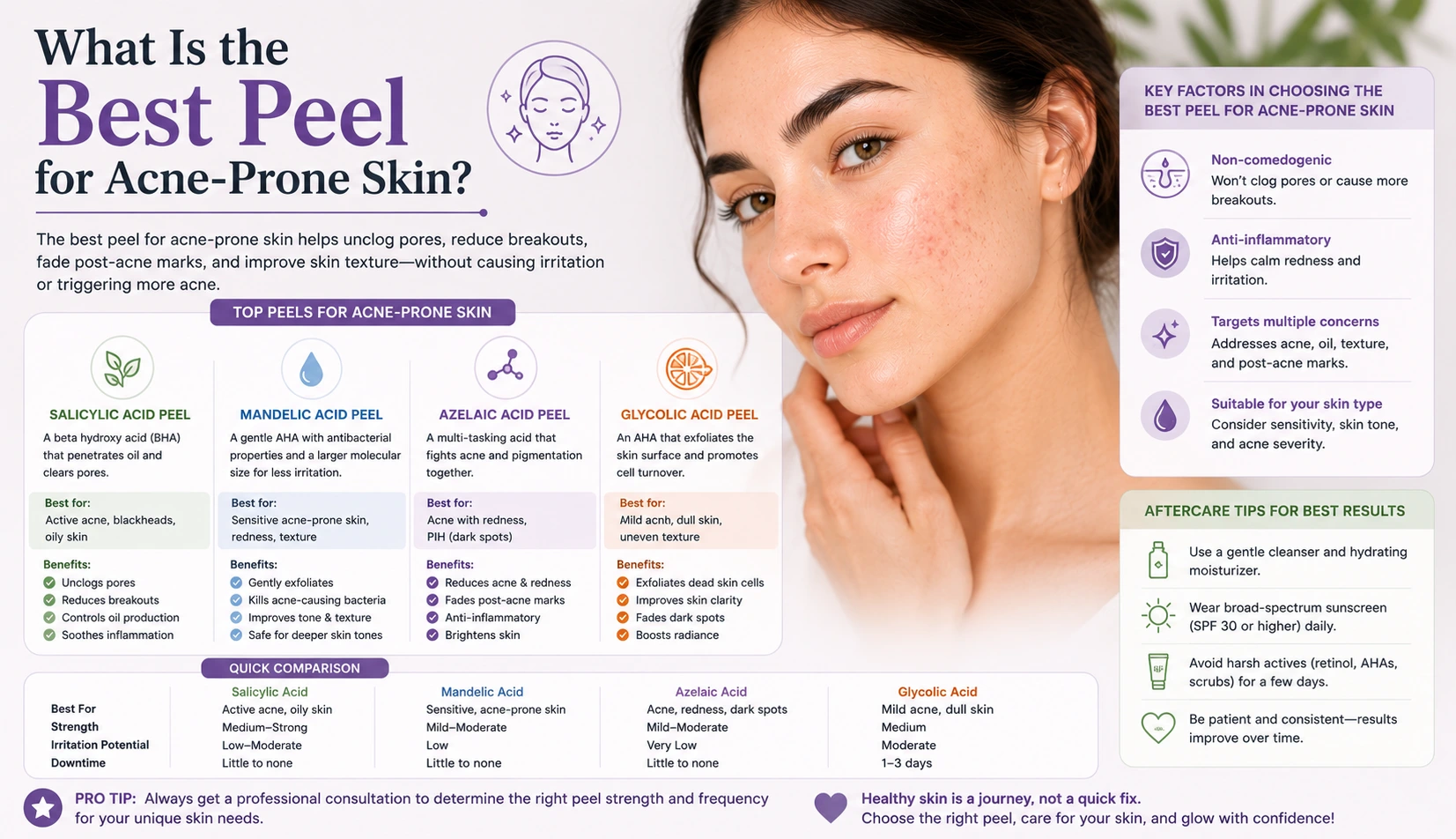
What Is the Best Peel for Acne-Prone Skin?
The best peel for acne-prone skin is one that supports meaningful cell turnover and skin renewal without generating the kind of inflammatory response that can trigger further breakout activity or worsen the post-inflammatory hyperpigmentation that so commonly accompanies acne. This immediately narrows the field. Acne-prone skin already lives with an elevated inflammatory baseline, and adding a significant chemical inflammatory load on top of it carries a real clinical risk of making the skin worse rather than better. For practitioners treating this client group and for clients researching their options, the mechanism of the peel is the first and most important consideration, before concentration, depth, or brand. A mechanical resurfacing approach, such as the Trexyne Peel, removes the chemical inflammatory trigger from the equation while still supporting the skin renewal and cell turnover that acne-prone skin needs. Understanding why that distinction matters clinically is the foundation of a good treatment decision.
Why Acne-Prone Skin Is Particularly Vulnerable to the Wrong Treatment
Acne-prone skin has characteristics that make it simultaneously in need of professional resurfacing and vulnerable to its most common risks. This is the central clinical tension practitioners face when treating this skin type, and it explains why treatment selection is more consequential here than for many other skin presentations.
Active acne involves recurring inflammatory events within the skin. Each inflamed lesion generates an inflammatory response that, in medium to darker skin tones, frequently produces post-inflammatory hyperpigmentation as it resolves. This combination of ongoing inflammation and PIH susceptibility means acne-prone skin is operating with a reduced threshold for inflammatory reactions and a demonstrated tendency to respond to inflammation with excess melanin production.
Applying a resurfacing treatment that generates a significant chemical inflammatory response to this skin type risks triggering two separate problems simultaneously: new or worsened breakout activity provoked by the inflammatory stimulus, and new PIH in the areas where that stimulus reaches susceptible melanocytes. In some clients, the result is skin that looks worse after treatment than before it, which understandably makes them reluctant to continue or try again.
The solution is not to avoid resurfacing. Acne-prone skin genuinely benefits from the accelerated cell turnover and surface renewal that professional resurfacing provides. The solution is to choose a resurfacing mechanism that achieves these outcomes without the chemical inflammatory burden that creates these risks.
The Role of Inflammation in Making Acne Worse
Understanding exactly how inflammation drives acne and PIH clarifies why minimising additional inflammatory stimulus during resurfacing is so important.
Acne develops when sebaceous glands overproduce sebum, dead skin cells accumulate within hair follicles, and the resulting environment allows the proliferation of bacteria that provoke an immune response. This immune response is the inflammation that produces the painful, visible lesions of inflammatory acne. The more significant the inflammatory response, the more likely it is to damage the surrounding skin tissue and produce PIH as the lesion heals.
A resurfacing treatment that adds to this inflammatory environment, by generating a chemical reaction in the skin that further activates inflammatory pathways, is not neutral in its effect on the underlying acne process. It introduces an additional inflammatory stimulus into skin that is already managing recurring inflammatory events, which can worsen the acne cycle rather than supporting its management alongside the skin quality improvements resurfacing is intended to deliver.
A mechanical resurfacing approach that does not engage this chemical inflammatory pathway is therefore not simply a gentler option. It is a clinically different option with a different risk profile for this specific skin type.
What Resurfacing Does for Acne-Prone Skin
When the mechanism is appropriate, professional resurfacing offers genuine clinical benefits for acne-prone skin that are worth articulating clearly to clients who may be uncertain whether any resurfacing treatment is suitable for them.
Accelerated cell turnover reduces the rate at which dead skin cells accumulate within follicles and contribute to congestion. By supporting more efficient shedding of the surface layers, resurfacing helps keep the pore environment cleaner and reduces one of the key factors that drives acne development.
Surface texture improvement addresses the uneven, congested quality that acne-prone skin often has even between breakouts. Rough, irregular texture reflects the accumulation of dead surface cells and subclinical congestion, and resurfacing progressively addresses both by stimulating consistent renewal across the treatment area.
PIH fading is the benefit many acne-prone clients are most directly seeking when they come for professional treatment. The dark marks left by previous breakouts can persist for months or years and are often more visible and more distressing than the active acne itself. Professional resurfacing accelerates the natural fading of these marks by stimulating cell turnover in the epidermal layers where the excess melanin sits.
How the Trexyne Peel Meets the Specific Needs of Acne-Prone Skin
The Trexyne Peel achieves resurfacing through marine-algae spicules that create controlled micro-channels in the skin surface through a purely mechanical mechanism. No chemical reaction takes place in the skin during treatment. The resurfacing stimulus is physical rather than chemical, which means the inflammatory pathway most directly associated with the risks described above is not engaged.
For acne-prone skin, this distinction has several practical clinical consequences. The risk of the treatment triggering further breakout activity is lower than with chemical resurfacing, because the chemical inflammatory stimulus is absent. The risk of producing new PIH in susceptible skin during treatment is reduced, because the chemical inflammatory trigger most directly associated with melanocyte overproduction in PIH-prone skin is not present. The recovery period involves a more predictable and manageable inflammatory response, which means acne-prone clients who are already managing their skin carefully can plan around the treatment more reliably.
The stabilised Vitamin E in the formulation supports the skin’s recovery phase from the first application. For acne-prone skin where the recovery window can be a period of elevated vulnerability, this recovery support reduces the residual inflammatory load during inter-session periods. The tiered protocol allows the practitioner to match intensity to the skin’s current condition at each session, which matters practically for a skin type that can present very differently from one appointment to the next depending on breakout activity and hormonal cycles.
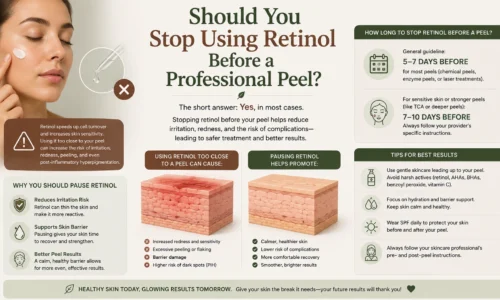
Timing: When Not to Treat Acne-Prone Skin
The best peel for acne-prone skin is also one applied at the right time, and this is a clinical judgement that must be made at each session rather than assumed to be constant throughout a course. Resurfacing should not be applied to skin with active, inflamed lesions in the treatment area, regardless of which peel is being used.
Treating over active breakouts risks spreading bacteria across the treatment area, disrupting active lesions, and generating an inflammatory response that compounds the existing acne inflammation rather than addressing the skin quality concerns the treatment is intended for. Deferring a session by one to two weeks when active lesions are present is always the correct clinical decision, even when it disrupts the preferred treatment schedule.
This is why the tiered protocol’s flexibility is particularly valuable for acne-prone clients. The ability to adjust not only intensity but also the decision to proceed at each appointment, based on how the skin actually presents rather than on a predetermined schedule, means the course can be managed responsively rather than rigidly.
Managing PIH Alongside Active Acne Management
Many clients presenting for professional resurfacing for acne-related PIH are also still managing active or recently resolved acne. These two elements of the concern need to be addressed as a connected system rather than in isolation.
If active acne is ongoing and uncontrolled during a resurfacing course, new PIH marks will continue to be produced by new breakouts even as existing marks are being addressed through resurfacing. The net effect can be a plateau in results where the resurfacing is clearing old marks but new ones appear at a similar rate. For these clients, integrating appropriate acne management, whether through a GP or dermatologist for prescription options, or through appropriate professional skincare advice, alongside the resurfacing course improves outcomes significantly.
If active acne is well controlled or has recently resolved by the time resurfacing begins, the course addresses the accumulated PIH without the complicating factor of new pigmentation being produced. This is the most favourable clinical scenario and typically produces the clearest, most consistent results.
Practitioners looking to incorporate the Trexyne Peel into their acne-prone skin treatment protocols can explore the full range through the Trexyne shop, or contact the team directly through the Trexyne contact page.
Expectations and Communication for Acne-Prone Clients
Acne-prone clients often come to professional treatment having already tried and been disappointed by a range of approaches. They may be cautious, frustrated, or both. Clear, honest communication about what this treatment can and cannot do, and what they are likely to experience in the early sessions, is essential for building the trust and compliance that determines whether a course produces good results.
Key messages to communicate include that improvement in PIH and surface quality builds progressively across a course rather than appearing quickly after one session, that some temporary purging of subclinical congestion is normal in the early sessions and does not mean the treatment is not working, that active breakouts will cause sessions to be deferred occasionally and this is a clinical necessity rather than a setback, and that daily SPF is a non-negotiable requirement for PIH improvement to proceed at its potential rate.
Clients who understand these realities are more likely to commit fully to the course, follow aftercare consistently, and evaluate their results accurately rather than abandoning treatment at the moment when it is just beginning to produce visible progress.
More information on the Trexyne approach to professional botanical resurfacing is available on the Trexyne website.
Conclusion
The best peel for acne-prone skin is a mechanical one that achieves meaningful cell turnover and skin renewal without the chemical inflammatory trigger that risks worsening breakout activity and post-inflammatory pigmentation in susceptible skin. Chemical resurfacing generates inflammation as part of its mechanism, which adds to the inflammatory burden that acne-prone skin is already managing and carries a documented risk of treatment-induced PIH in medium to darker skin tones. The Trexyne Peel resurfaces through marine-algae spicules without chemical exfoliants, includes stabilised Vitamin E to support recovery, and uses a tiered protocol that adapts to the variable condition of acne-prone skin across sessions. Applied at the right time in the skin’s cycle, with appropriate session spacing, consistent daily SPF, and honest expectation-setting from the outset, it may support a meaningful, progressive improvement in surface quality, congestion, and PIH, contributing to a clearer, more even-looking complexion for clients whose acne-prone skin needs a carefully matched resurfacing approach.
FAQs
Q: What is the best type of peel for acne-prone skin?
A mechanical peel that achieves cell turnover without generating a chemical inflammatory response is generally better suited to acne-prone skin than chemical resurfacing. Chemical peels add inflammatory stimulus to skin that already has an elevated inflammatory baseline from acne, which can worsen breakout activity and trigger post-inflammatory pigmentation. A mechanical approach removes this specific risk.
Q: Can the Trexyne Peel help acne-prone skin?
Yes. The Trexyne Peel supports cell turnover through a purely mechanical mechanism, addressing congestion, surface texture, and post-inflammatory pigmentation without the chemical inflammatory trigger most likely to worsen acne-related concerns. The tiered protocol adapts to the variable condition of acne-prone skin at each session, and resurfacing is deferred when active inflamed lesions are present.
Q: Will a professional peel make acne worse?
Applied correctly and at the right time, a professional peel should not make acne worse. Resurfacing should never be applied over active, inflamed lesions. Some clients experience temporary purging of existing subclinical congestion in the early sessions, which is different from new acne being caused by the treatment. A mechanical peel carries a lower risk of worsening acne than a chemical approach that generates significant inflammation.
Q: Should I treat my acne before having a peel for PIH?
Getting active acne to a controlled or manageable level before beginning a resurfacing course for PIH produces the best results, because new breakouts during the course create new PIH at the same time as resurfacing is addressing existing marks. Fully resolving acne before starting is ideal; managing it adequately so new lesions are infrequent during the course is a practical minimum.
Q: How many sessions of the Trexyne Peel are needed for acne-related PIH?
PIH improvement builds progressively across a course, with more noticeable fading typically apparent from the third or fourth session onwards. The total number of sessions depends on the depth and age of the marks, how actively the acne is being managed during the course, and how consistently daily SPF is maintained. A practitioner assessment provides a realistic recommendation.
Q: Is daily SPF important for acne-prone skin having a professional peel?
Yes. Daily SPF is essential for PIH fading to proceed at its potential rate. UV exposure stimulates melanocyte activity in areas affected by PIH, deepening existing marks and slowing visible progress. For acne-prone skin that is also PIH-susceptible, consistent daily photoprotection throughout the resurfacing course is a clinical requirement rather than optional advice.
Q: Can I have the Trexyne Peel if I am using prescription acne medication?
Some prescription acne treatments affect skin sensitivity and barrier function in ways that are relevant to how resurfacing is timed and managed. This should be disclosed at consultation so the practitioner can make an informed decision about appropriate intensity and timing. Certain medications require a defined waiting period before resurfacing is appropriate. A thorough consultation before any session begins is essential for clients on prescription acne treatment.