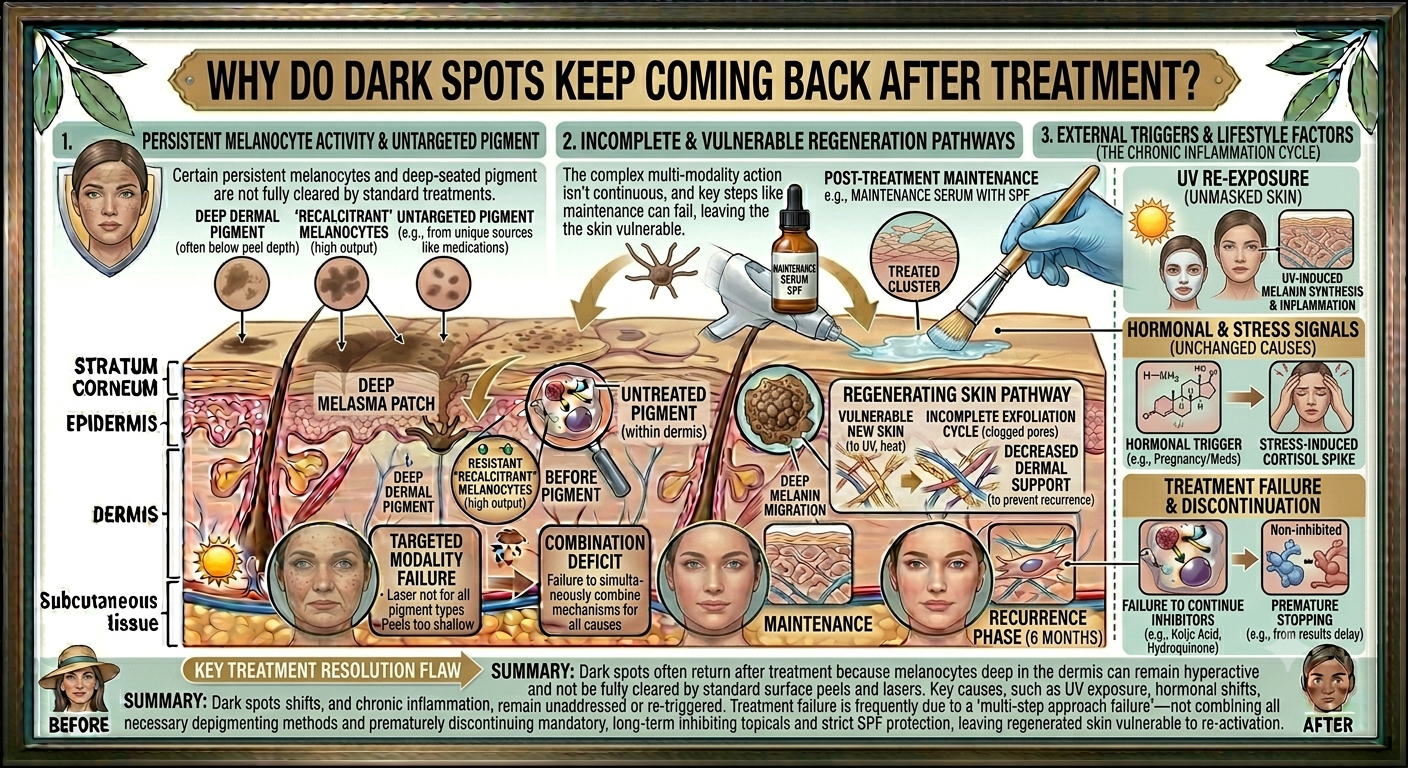
Why Do Dark Spots Keep Coming Back After Treatment
If dark spots keep returning after treatment, the treatment itself probably is not the problem. The more likely explanation is that the underlying triggers are still active. Pigmentation is a symptom of something happening in the skin — UV exposure, inflammation, hormonal activity, or a combination of all three. Treat the surface without addressing those drivers and the spots will come back, often within weeks. Understanding why recurrence happens is the foundation of any resurfacing programme that actually holds its results. For practitioners building a longer-term approach, the Trexyne Peel — Professional Algae Resurfacing Treatment offers a botanical, mechanically driven option that supports skin renewal as part of a considered, ongoing strategy.
The Real Reason Dark Spots Return
Most clients who experience recurring pigmentation assume the treatment stopped working. In practice, what has usually happened is that one or more of the original triggers has gone unaddressed. The skin cleared, the client eased off their protective routine, and the melanocytes got to work again.
Melanocytes do not switch off after treatment. They respond to their environment continuously. UV radiation, inflammation, and hormonal signals can all stimulate them at any point. Resurfacing treatments remove existing pigmented cells. They do not permanently reset the melanocytes producing new ones. This is the central reality that shapes every honest conversation about pigmentation management.
UV Exposure: The Most Consistent Trigger
UV radiation is the dominant driver of hyperpigmentation recurrence. The biology is straightforward. UV light stimulates melanocytes to produce melanin as a protective response. In skin that is prone to uneven pigmentation, that response tends to be exaggerated and localised.
After a resurfacing course, the skin surface is clearer. But if SPF compliance drops, those same melanocytes are still sitting in the epidermis, ready to respond. A few weeks of sun exposure without adequate protection is often all it takes to undo several sessions of progress.
The SPF Compliance Gap
This is one of the most common points of failure in pigmentation management. Clients who are motivated during a treatment course often relax their sun protection habits once they see improvement. The very success of the treatment can create a false sense of security.
SPF 30 is the clinical minimum. SPF 50 is more appropriate for clients with active pigmentation concerns, those spending time outdoors, or those in summer months. Reapplication is not optional. Wearing SPF once in the morning and spending the afternoon outdoors without reapplying is not meaningful sun protection. This conversation needs to happen at every appointment, not just the first one.
Inflammation: The Hidden Perpetuator
Post-inflammatory hyperpigmentation is one of the most common forms of recurrent pigmentation seen in clinic. It develops after any skin trauma that triggers a localised inflammatory response. Acne breakouts are the most frequent culprit, but anything from minor abrasion to overly aggressive skincare routines can set it off.
The frustrating pattern for many clients is that treating the acne clears the breakouts, the resurfacing programme fades the existing PIH, and then a new breakout appears and the cycle starts again. Unless the underlying acne is properly managed, the pigmentation will keep recurring regardless of how well the resurfacing works.
Skincare-Induced Inflammation
Overly aggressive home skincare is another common but under-discussed trigger. Clients who apply multiple active products without professional guidance can create a chronic low-level inflammatory state that keeps stimulating melanin production. Strong physical scrubs, high-frequency exfoliants used too often, and layering actives without knowledge of interactions can all contribute.
Part of the practitioner’s role is reviewing what the client is using at home and identifying whether anything in their routine could be perpetuating the problem.
Hormonal Drivers: The Recurring Pattern That Won’t Quit
Hormonal hyperpigmentation, most commonly melasma, behaves differently from sun spots or PIH. It tends to be more diffuse, more symmetrical, and more resistant to resurfacing alone. It also recurs reliably if the hormonal environment remains unchanged.
How Oestrogen Influences Pigmentation
Elevated oestrogen levels are strongly associated with increased melanocyte activity. This is why melasma is particularly common during pregnancy, and why some clients find their pigmentation flares in the days before menstruation or after starting hormonal contraception. These hormonal fluctuations do not stop because the skin has been resurfaced.
For clients with melasma, resurfacing may improve the visible appearance of surface pigmentation, but the underlying hormonal driver remains. This means the treatment conversation has to include a clear explanation of why maintenance is not optional. It also means that expectations need to be calibrated to the reality of the condition rather than to the hope of a permanent solution.
Why Resurfacing Alone Is Not Enough for Lasting Results
Resurfacing treatments work by accelerating cell turnover and encouraging pigmented cells to shed. They can produce impressive visible results over a course of treatments. But they address the skin’s current state, not the conditions that will shape its future state.
This is why a resurfacing programme works best as part of a wider strategy. The treatment clears existing pigmentation. The practitioner-guided home care, SPF compliance, and trigger management work to slow the rate at which new pigmentation forms. Without that second layer, the improvements tend to be temporary.
The Trexyne Peel is designed to support skin renewal through a mechanical mechanism using marine algae spicules. These microscopic structures create controlled micro-channels in the skin without chemical exfoliants, stimulating a renewal response that progressively improves the look of uneven tone. Stabilised Vitamin E in the formulation may support the skin’s recovery phase. But the treatment works best when the practitioner is also actively managing the triggers that drive recurrence.
The Case for Maintenance Treatment
Clients who achieve good results and then stop treatment entirely are the most likely to experience significant recurrence. This is not a flaw in the treatment. It is the nature of conditions like PIH, solar lentigines, and melasma. The skin’s pigmentation behaviour is ongoing. Management needs to match that reality.
Building Maintenance Into the Programme
A practical approach is to transition clients from an active treatment course to a maintenance schedule once visible improvement has been achieved. Less frequent sessions keep the renewal process ticking over and catch early pigmentation before it becomes established again.
The Trexyne Peel’s tiered protocol supports this well. Intensity can be reduced for maintenance sessions compared to the initial clearing phase, which is both kinder to the skin and easier to fit into a client’s schedule. You can view available pack sizes and plan accordingly via the Trexyne shop.
How to Have the Recurrence Conversation With Clients
Managing client expectations is part of managing their skin. Clients who understand why recurrence happens are more likely to stick with their SPF routine, maintain their appointment schedule, and report early signs of pigmentation returning rather than waiting until it is well established again.
The key points to communicate clearly:
The treatment removes existing pigmentation. It does not stop the skin from producing new pigmentation in response to UV, inflammation, or hormonal activity. SPF is as important as the treatment itself in maintaining results. Maintenance appointments are part of the programme, not an optional extra. Recurrence is not a failure. It is the skin responding to its environment, which is manageable with the right ongoing approach.
Framing this well at the outset saves a lot of difficult conversations later when a client returns frustrated that their spots have come back.
Identifying Which Trigger Is Driving Recurrence
When a client returns with pigmentation recurring after a successful treatment course, the first step is working out what has changed or what was never fully addressed. A few targeted questions usually get to the root of it.
Have they been consistent with SPF? Where are the spots recurring, and is the pattern the same as before or different? Has anything changed in their skincare routine or lifestyle? For female clients, have there been any hormonal changes, including contraception, pregnancy, or menstrual cycle patterns? Have they had any new inflammatory events, such as acne or skin irritation?
The answers to these questions shape the next stage of the treatment plan. Returning to resurfacing without addressing the trigger is likely to produce the same cycle of improvement and recurrence.
What a Recurrence-Resistant Programme Looks Like
The most effective pigmentation programmes tend to combine several elements rather than relying on resurfacing alone.
Professional resurfacing sessions at appropriate intervals form the core of the plan. The Trexyne Peel’s mechanical approach makes it a suitable choice for clients where minimising the risk of treatment-induced inflammation is a priority. Its predictable downtime and tiered protocol allow intensity to be matched to the client’s skin and history at each visit.
SPF compliance is non-negotiable and reinforced consistently. Home skincare is reviewed and simplified where over-application of actives may be causing low-level inflammation. Lifestyle factors including heat exposure, stress, and skincare habits are discussed openly. For clients with suspected hormonal drivers, a referral to a GP or specialist may be appropriate alongside the aesthetic programme.
For practitioners who want to discuss how the Trexyne Peel fits into this kind of approach for their clinic, the team is available to help via the contact page.
The Fitzpatrick Factor: Why Skin Tone Affects Recurrence Risk
Clients with medium to deeper skin tones tend to experience more pronounced recurrence. Melanocytes in these skin types are more reactive to stimulation, which means the same level of UV exposure, inflammation, or hormonal trigger can produce a stronger pigmentation response than in lighter skin tones.
This does not mean resurfacing cannot be effective. It means the treatment protocol needs to be more conservative and the trigger management more rigorous. Lower intensity at the outset, longer intervals between sessions, and absolute commitment to SPF compliance are all part of managing pigmentation in Fitzpatrick IV through VI skin.
The mechanical nature of the Trexyne Peel, combined with its absence of chemical exfoliants, may reduce the risk of treatment-induced PIH in this context. That said, individual assessment remains essential, and no protocol should be applied without proper consultation and patch testing. More information on the Trexyne Peel’s professional framework is available at Trexyne.com.
Conclusion
Dark spots return after treatment because the conditions that created them in the first place continue to operate. UV exposure keeps stimulating melanocytes. Inflammation from ongoing acne or reactive skincare routines keeps triggering PIH. Hormonal fluctuations keep driving melasma. Resurfacing clears what is there now, but it does not switch off the mechanisms that produce new pigmentation.
Managing recurrence means treating the skin’s current state and the drivers that will shape its future. The Trexyne Peel supports skin renewal through a botanical, mechanical mechanism that may help progressively improve the appearance of uneven tone over a structured course of treatment. With stabilised Vitamin E to support recovery and a tiered protocol that adapts to individual skin profiles, it sits well within a longer-term pigmentation management plan. Paired with consistent SPF use, appropriate home care, and clear client communication about the ongoing nature of pigmentation, it offers practitioners a considered and reliable tool for helping clients achieve and maintain a brighter, more even-looking complexion.
Frequently Asked Questions
Q: Why do dark spots come back after a professional skin treatment?
Dark spots return when the underlying triggers remain active. Resurfacing treatments clear existing pigmented cells, but melanocytes continue responding to UV, inflammation, and hormonal signals. If sun protection lapses, if inflammatory breakouts continue, or if hormonal drivers are not managed, new pigmentation will form regardless of how effective the treatment was. Maintenance treatment and consistent SPF use are both essential to sustaining results.
Q: How can I stop dark spots from returning after a peel?
The most effective approach combines ongoing professional resurfacing with strict SPF compliance, a reviewed and appropriately simplified home skincare routine, and active management of known triggers like acne or hormonal fluctuations. A single treatment course without these supporting measures is unlikely to produce lasting results. Practitioners often recommend transitioning clients from an active course to a maintenance schedule to keep pigmentation from re-establishing.
Q: Is melasma likely to come back after resurfacing treatment?
Melasma has a strong tendency to recur because its hormonal drivers remain active. Resurfacing may improve the visible appearance of surface pigmentation, but it does not address the underlying cause. Clients with melasma benefit from a management plan that includes SPF compliance, awareness of hormonal triggers, and realistic expectations about ongoing maintenance rather than a permanent solution.
Q: How does the Trexyne Peel support long-term pigmentation management?
The Trexyne Peel uses marine algae spicules to create controlled micro-channels in the skin through a purely mechanical mechanism, stimulating cell renewal and supporting the gradual improvement of uneven tone. Its tiered protocol allows intensity to be adjusted across a course, which suits both active treatment phases and lower-intensity maintenance sessions. The stabilised Vitamin E in the formulation may also support skin recovery between appointments, helping the skin maintain its renewal response over time.
Q: Can recurring PIH be treated effectively with a botanical peel?
Post-inflammatory hyperpigmentation that keeps recurring is usually linked to an ongoing source of inflammation, most commonly active acne. A botanical peel like the Trexyne Peel may support the progressive improvement of surface PIH, but the underlying inflammatory trigger needs to be managed simultaneously. Without addressing what is causing the inflammation, new PIH is likely to form at a rate that outpaces the resurfacing.
Q: How often should maintenance peel treatments be scheduled for recurring dark spots?
The right interval depends on the type of pigmentation, the client’s skin profile, and how quickly pigmentation tends to re-emerge after treatment. Maintenance sessions are typically less frequent and lower in intensity than the initial clearing course. The Trexyne Peel’s tiered protocol supports this kind of adaptive scheduling. Practitioners can discuss appropriate intervals for their clients’ specific needs with the Trexyne team via the contact page.
Q: Is it safe to continue resurfacing treatment on skin that keeps producing dark spots?
Generally, yes, provided the treatment protocol is appropriate for the skin type and the triggers are being addressed. For clients with hyperpigmentation-prone skin, the mechanical approach of the Trexyne Peel may be preferable because it avoids the risk of treatment-induced inflammation that can perpetuate PIH. Conservative protocols, patch testing, and thorough skin assessment at each visit remain important, particularly for clients with Fitzpatrick skin types IV and above.